
Articles
- Page Path
- HOME > J Prev Med Public Health > Volume 57(1); 2024 > Article
-
Original Article
Changes in Adolescent Health Behavior and the Exacerbation of Economic Hardship During the COVID-19 Pandemic: A Cross-sectional Study From the Korea Youth Risk Behavior Survey -
Chaeeun Kim1
 , Haeun Lee1, Kyunghee Jung-Choi2
, Haeun Lee1, Kyunghee Jung-Choi2 , Hyesook Park3
, Hyesook Park3 -
Journal of Preventive Medicine and Public Health 2024;57(1):18-27.
DOI: https://doi.org/10.3961/jpmph.23.306
Published online: November 11, 2023
- 1,371 Views
- 170 Download
1Ewha Womans University College of Medicine, Seoul, Korea
2Department of Environmental Medicine, Ewha Womans University College of Medicine, Seoul, Korea
3Department of Preventive Medicine, Graduate Program in Health System Science & Engineering, Ewha Womans University College of Medicine, Seoul, Korea
- Corresponding author: Hyesook Park, Department of Preventive Medicine, Graduate Program in Health System Science & Engineering, Ewha Womans University College of Medicine, 25 Magokdong-ro 2-gil, Gangseo-gu, Seoul 07804, Korea E-mail: hpark@ewha.ac.kr
- Co-corresponding author: Kyunghee Jung-Choi, Department of Environmental Medicine, Ewha Womans University College of Medicine, 25 Magokdong-ro 2-gil, Gangseo-gu, Seoul 07804, Korea E-mail: jungchoi@ewha.ac.kr
Copyright © 2024 The Korean Society for Preventive Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Objectives:
- This study investigated the association between exacerbated economic hardship during the coronavirus disease 2019 (COVID-19) pandemic and changes in the health behaviors of Korean adolescents.
-
Methods:
- We analyzed data from the 2021 Korea Youth Risk Behavior Survey and included 44 908 students (22 823 boys and 22 085 girls) as study subjects. The dependent variables included changes in health behaviors (breakfast habits, physical activity, and alcohol use) that occurred during the COVID-19 pandemic. The aggravation of economic hardship by COVID-19 and the subjective economic status of the family were used as exposure variables. Multiple logistic regression analysis was utilized to calculate the prevalence odds ratios (PORs).
-
Results:
- Severe exacerbation of a family’s economic hardship due to COVID-19 was negatively associated with the health behaviors of adolescents, including increased breakfast skipping (POR, 1.85; 95% confidence interval [CI], 1.55 to 2.21 for boys and POR, 1.56; 95% CI, 1.27 to 1.92 for girls) and decreased physical activity (POR, 1.37; 95% CI, 1.19 to 1.57 for boys and POR, 1.38; 95% CI, 1.19 to 1.60 for girls). These negative changes in health behaviors were further amplified when combined with a low subjective family economic status.
-
Conclusions:
- The experience of worsening household hardship can lead to negative changes in health behavior among adolescents. It is crucial to implement measures that address the economic challenges that arise from stressful events such as COVID-19 and to strive to improve the lifestyles of adolescents under such circumstances.
- Coronavirus disease 2019 (COVID-19) emerged in late 2019 and led to a global pandemic by March 2020 [1]. In response to this unprecedented situation, countries worldwide, including Korea, implemented various measures to protect their populations. The Korean government responded to the uncertain pandemic situation with comprehensive measures such as social distancing, quarantines, prompt diagnostic testing, contact tracing, timely treatment, and vaccination [2]. Social distancing measures included stay-at-home orders and the closure of schools; thus, Korean adolescents had to adapt to online classes at home. Furthermore, the public institutions and academies that were primary venues for after-school activities became unavailable or operated with a limited capacity. The impact of COVID-19 on the daily lives of Korean adolescents raised concerns regarding their physical and mental health [3].
- In addition to the social impacts of the COVID-19 pandemic, the economic repercussions could not be ignored. The 2020 economic shock was comparable to the 2008 global financial crisis, with a 3.7% decline in the growth rate of the gross domestic product and a 7.4% decrease in the private consumption growth rate [4]. That same year, 460 000 Koreans lost their jobs [4]. Many people, particularly temporary or per diem workers in the manufacturing sector and self-employed people with employees, faced challenges related to unemployment. Adolescents also suffered the consequences of these economic impacts.
- Studies reported an increased prevalence of obesity and overweight among adolescents during the pandemic [5], as well as an increased prevalence of anxiety when families experienced economic difficulties due to COVID-19 [6]. Smartphone usage and alcohol consumption among adolescents increased during the pandemic, particularly in families experiencing economic difficulties [7,8]. These findings suggest that COVID-19 significantly affected the daily lives of Korean adolescents and that the alterations in household economic status because of COVID-19 influenced their lifestyle habits.
- Despite investigations into the health and health behaviors of adolescents before and during the COVID-19 pandemic, comprehensive research on how changes in household economic status affected their lifestyle habits remains limited. Most studies have focused on the relationship between adolescents’ mental health and family economic conditions. Furthermore, studies that simultaneously evaluated the dynamic factors of adolescents’ health behaviors and their economic difficulties were scarce. Therefore, the present study explored the association between family economic adversity following COVID-19 and changes in the health behaviors of Korean adolescents using nationally representative data. In addition, we assessed the combined associations of exacerbated family economic hardship and subjective family economic status on changes in health behaviors.
INTRODUCTION
- Materials
- The Korea Youth Risk Behavior Survey (KYRBS) is a joint initiative of the Korea Centers for Disease Control and Prevention and the Ministry of Education. The survey gathers statistics on the health behaviors of Korean adolescents. It is an anonymous, self-reported online survey conducted annually since 2005 for middle school and high school students nationwide. The survey results serve as a basis for the planning and evaluation of youth health policies and health promotion projects [9].
- This study was a cross-sectional study using data from the 2021 KYRBS. Using a complex sampling method, one class per grade from 400 middle schools and 400 high schools across the country was selected. The survey consisted of questions on adolescent health behaviors such as smoking, drinking, and physical activity, and additional questions were added in 2021 on health equity and the changes in daily life before and during the COVID-19 pandemic. The survey was performed between August 2021 and November 2021, with a teacher supervising students as they accessed the KYRBS website to participate. A total of 54 848 students from 399 middle schools and 397 high schools participated in the survey. From that total, the present study analyzed 44 908 students (22 823 boys and 22 085 girls), excluding those who did not respond to the questions on lifestyle factors or household income.
- Dependent Variables
- The dependent variables were lifestyle changes in breakfast habits, physical activity, and alcohol use that occurred during the COVID-19 pandemic. To determine the negative impact of COVID-19 on daily lifestyle, we analyzed whether the students skipped breakfast more often, had decreased physical activity, or had an increased consumption of alcohol. Responses to the question “Compared to before the COVID-19 pandemic, what changes have you made?” were used to classify changes in breakfast habits, physical activity, and alcohol use. We classified skipping breakfast or drinking alcohol as increased for the responses “strongly increased” or “increased” and labeled physical activity as decreased for the responses “decreased” or “strongly decreased.” Reference values were derived from the combined responses of “none,” “decreased,” or “strongly decreased.” Smoking was not included as a dependent variable because of the limited number of respondents who reported smoking and the large number of missing values.
- Exposure Variables
- The change in economic level during the COVID-19 pandemic and the subjective family economic status were used as exposure variables. The change in economic status during the COVID-19 pandemic was based on answers to the question “To what degree has your family’s economic status become more difficult than before COVID-19?” Answers included “severe,” “moderate,” “slight,” or “none.” For answers to the question “What is the economic status of your family?” the subjective family economic status was classified as high for those who responded “high” or “middle-high,” middle for those who responded “middle,” and low for those who responded “middle-low” or “low.”
- Covariates
- In this study, we adjusted for grade level, residential area, whether residing with parents, subjective health status, and depression status. Additional adjustments were made for each outcome variable. Differences between weekday and weekend wake-up times were also adjusted for the analysis of breakfast skipping. For the analysis of physical activity, additional adjustments were made for the average smartphone usage (time per day) and the average time per day spent sitting down. For alcohol use, smoking status was also adjusted.
- Subjective health status was categorized into 3 groups: healthy, moderate, and unhealthy. Depressive status was classified as no or yes, based on the presence or absence of depressed mood over the past 12 months. To analyze the regularity of wake-up times, we considered the difference between weekday and weekend wake-up times for all study subjects and grouped them into 2 categories: the average group and the non-average group. The non-average group was determined based on criteria related to the mean plus standard deviation of each variable. Specifically, we categorized the difference between the average weekday versus weekend wake-up times as either ≥5 hours or <5 hours. The average daily smartphone usage was classified into 2 groups: those who used their smartphones ≥8.5 hours and those who used them <8.5 hours. Similarly, we divided the average time per day spent sitting down into 2 groups: ≥15 hours and <15 hours.
- Statistical Analysis
- To assess the impact of changes in the level of economic hardship and subjective family economic status on lifestyle changes during the COVID-19 pandemic, we used multiple logistic regression analysis to calculate the prevalence odds ratios (PORs). Initially, we evaluated the association between each exposure variable and the lifestyle changes during the COVID-19 pandemic, adjusting for covariates. Subsequently, we created 12 groups by combining COVID-19-related family economic hardship and subjective family economic status as exposure variables and conducted logistic regression analysis. The results of those analyses were presented as crude and adjusted PORs with corresponding 95% confidence intervals (CIs). In the statistical analysis we accounted for the complex sampling method utilized in the KYRBS. All statistical analyses were performed using R version 4.3.1 (R Foundation for Statistical Computing, Vienna, Austria) with α = 0.05.
- Ethics Statement
- This study used only a de-identified database disclosed to the public without personal identification information; therefore, neither approval by the institutional review board nor obtainment of the informed consent is necessary.
METHODS
- The general characteristics of the study subjects are presented in Table 1 and Supplemental Material 1. COVID-19-related family economic hardship was reported as severe and moderate by 5.4% and 24.5% of boys, respectively, and was reported as severe and moderate by 4.5% and 23.8% of girls, respectively. Regarding subjective family economic status, 10.7% of boys responded that it was low, 47.5% that it was middle, and 41.8% that it was high. Among girls, the corresponding figures were 9.9% for low, 52.2% for middle, and 37.9% for high. After the COVID-19 pandemic, 13.1% of boys and 13.6% of girls skipped breakfast more often than before the pandemic. In addition, 43.1% of boys and 57.3% of girls described a decrease in physical activity. Alcohol consumption was increased following the pandemic in 2.1% of boys and 1.7% of girls. Both boys and girls who reported severe COVID-19-related family economic adversity exhibited the highest rate of skipping breakfast (19.2% in boys and 18.1% in girls) as well as the largest percentage to report a decline in physical activity (47.8% of boys and 62.1% of girls) and an increase in alcohol consumption (3.3% of boys and 3.6% of girls).
- Logistic regression analysis was used to examine the relationship between COVID-19-related economic hardship and the dependent variables, and the results are presented in Table 2. There was a significant difference in breakfast skipping according to the degree of COVID-19-related economic difficulty, whereas no significant differences in breakfast skipping were determined by subjective family economic status. Among boys, the severity of COVID-19-related economic hardship was positively correlated with an increase in skipping breakfast (POR, 1.12; 95% CI, 1.01 to 1.25 for “slight”; POR, 1.40; 95% CI, 1.25 to 1.57 for “moderate”; and POR, 1.85; 95% CI, 1.55 to 2.21 for “severe”; p for trend <0.001). The same trend was observed among girls (POR, 1.06; 95% CI, 0.95 to 1.19 for “slight”; POR, 1.30; 95% CI, 1.15 to 1.48 for “moderate”; and POR, 1.56; 95% CI, 1.27 to 1.92 for “severe”; p for trend <0.001).
- As with the increases in skipping breakfast, there was no statistically significant difference in the extent of decreased physical activity based on subjective family economic status for girls, but not for boys. However, a statistically significant difference was found between groups for decreased physical activity based on the degree of COVID-19-related family economic hardship. As the degree of COVID-19-related family economic hardship increased from “none” to “severe” for both boys and girls, there was a corresponding increase in the magnitude of the association with decreased physical activity among boys (POR, 1.11; 95% CI, 1.03 to 1.19 for “slight”; POR, 1.20; 95% CI, 1.11 to 1.31 for “moderate”; and POR, 1.37; 95% CI, 1.19 to 1.57 for “severe”) and among girls (POR, 1.11; 95% CI, 1.04 to 1.18 for “slight”; POR, 1.26; 95% CI, 1.16 to 1.37 for “moderate”; and POR, 1.38; 95% CI, 1.19 to 1.60 for “severe”).
- In addition, there was no significant difference in increased alcohol consumption by groups based on the subjective family economic status for both boys and girls. As the hardship approached “severe”, those who reported increased drinking tended to be higher than the “none” group among both girls and boys (girls’ POR, 1.41; 95% CI, 0.81 to 2.47 for “severe”; and boys’ POR, 1.41; 95% CI, 0.91 to 2.20 for “severe”), although the difference was not significant.
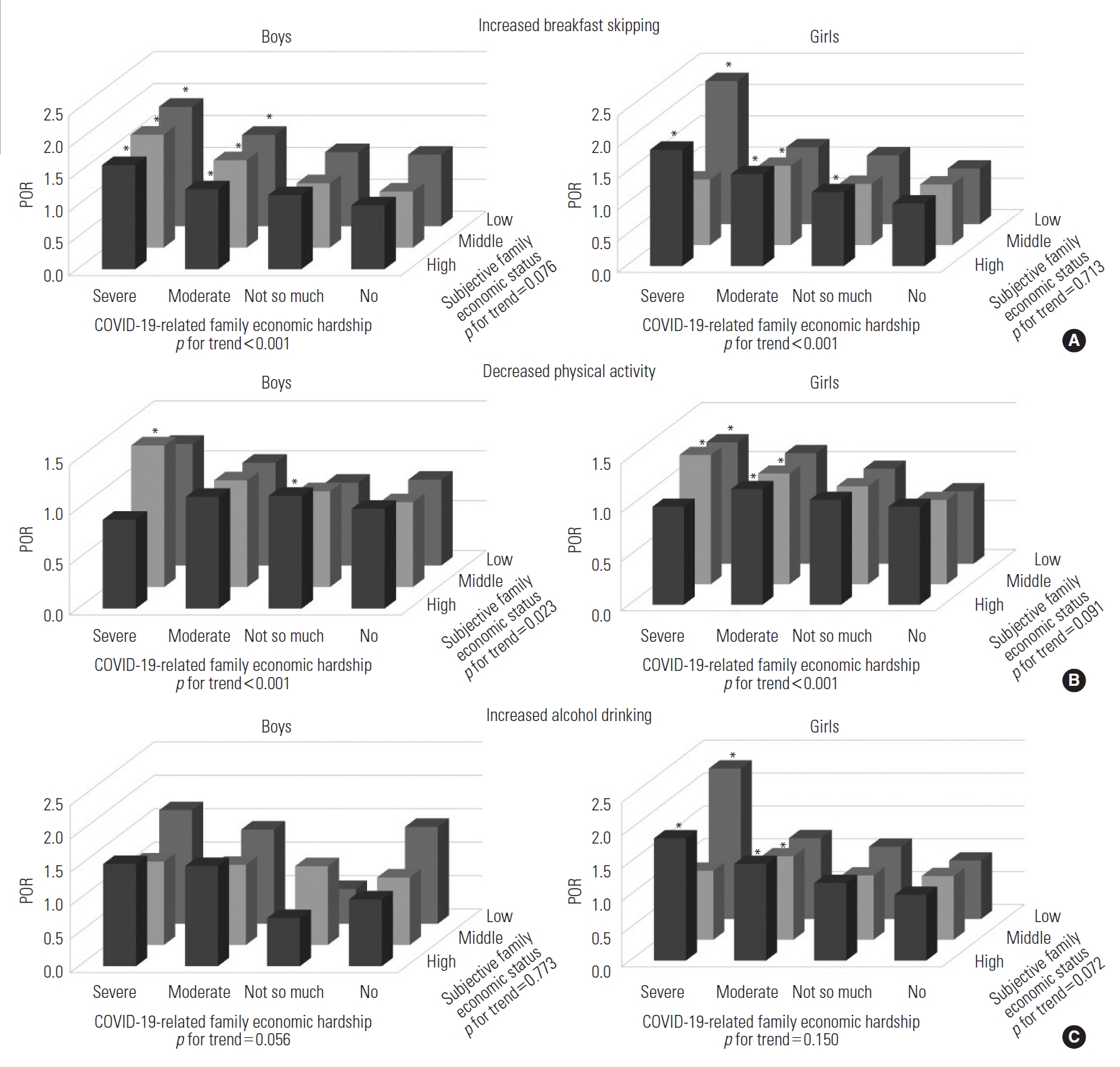
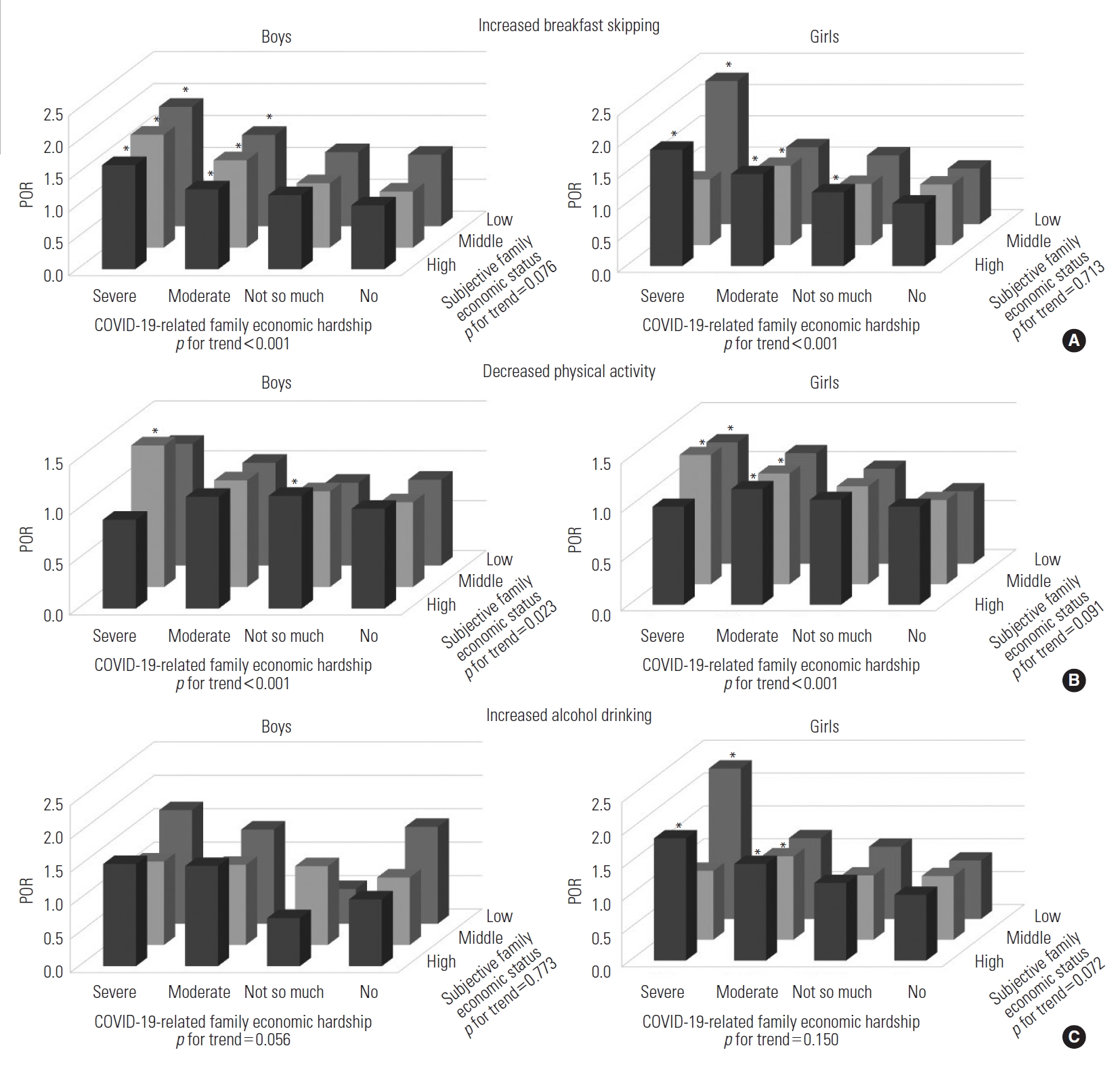
- The adjusted PORs of the dependent variables in the combined COVID-19-related family economic hardship and subjective family economic status categories for Korean adolescents are illustrated in Figure 1. Both male and female students who experienced severe economic difficulty during the COVID-19 pandemic and had a low subjective economic status had the highest risk for an increase in skipping breakfast (POR, 1.87; 95% CI, 1.42 to 2.47 for boys, and POR, 2.29; 95% CI, 1.71 to 3.08 for girls) (Supplemental Material 2). The risk of decreased physical activity was highest for boys and girls who faced severe economic hardship during the COVID-19 pandemic and were in a middle economic status (POR, 1.42; 95% CI, 1.16 to 1.73 for boys, and POR, 1.32; 95% CI, 1.05 to 1.66 for girls) (Supplemental Material 3). Female students who encountered severe economic hardship during the COVID-19 pandemic and had a low subjective economic status had the highest risk of increased alcohol consumption (POR, 2.29; 95% CI, 1.71 to 3.08) (Supplemental Material 4 and 5).
RESULTS
- This study revealed that family economic hardship due to the COVID-19 pandemic was negatively associated with adolescents’ health behaviors, including skipping breakfast, decreased physical activity, and increased alcohol consumption. These negative changes in health behaviors were further aggravated when combined with a low subjective family economic status.
- Eating breakfast in adolescence has positive effects on cognitive performance, academic achievement, quality of life, and well-being, while reducing the risk factors for morbidity [10]. However, there was an increasing trend in the proportion of middle and high school students who had not eaten breakfast for >4 days in the past 7 days: 27.9% in 2015, 35.7% in 2019, 37.3% in 2020, and 38.0% in 2021 [11]. Studies have reported socioeconomic inequalities in breakfast skipping among adolescents, with a higher tendency to skip breakfast among those with a lower perceived socioeconomic position (SEP). For example, in Spain, the lower tertile of SEP had approximately 1.3× higher odds of skipping breakfast than the higher tertile of SEP [12]. Similar findings were observed in previous studies conducted in Korea, where adolescents with a low subjective income level were more likely to skip breakfast [13].
- The COVID-19 pandemic had varying effects on dietary patterns [14]. We identified that negative changes in the family’s economic situation related to COVID-19 increased the frequency of skipping breakfast. This finding aligns with a previous study, which demonstrated that negative changes in household income have an undesirable impact on health behaviors such as smoking and problem behaviors [15,16]. A study conducted in the United Kingdom revealed that when subjective income levels decreased, the composition of children’s diets shifted towards less healthy foods [17]. This suggests that a decrease in income level not only affects the frequency of breakfast consumption but also the overall quality of breakfast at home. Therefore, to comprehend the impact of the economic difficulties caused by COVID-19, it is crucial to assess not only the number of breakfast meals but also changes in diet composition.
- With the outbreak of COVID-19, there was a notable decrease in physical activity among adolescents [3,18,19]. In our study, 43.1% of boys and 57.3% of girls reported a decrease in physical activity. These declines were more prevalent in families that experienced severe economic difficulties related to COVID-19. A study conducted in the United States also demonstrated a link between financial hardship during the pandemic and reduced exercise, consistent with our findings [20]. The stressful circumstances brought on by both financial difficulties and the COVID-19 pandemic could result in less physical exercise [20]. Conversely, physical activity plays a significant role in promoting mental health. Engaging in long-term physical activity can enhance students’ self-efficacy [21], and their school years are a particularly important time for mental development and the cultivation of high self-efficacy [22]. Previous research has also shown that economic difficulties tend to decrease students’ self-efficacy [23]. Therefore, it is essential to provide students, especially those with low or decreased economic status, with opportunities to restore their self-efficacy through physical activity [24].
- The prevalence of alcohol use among Korean adolescents decreased during the COVID-19 pandemic [25]. Meanwhile, our study found that adolescents facing economic hardship related to COVID-19 had a higher risk of increasing their alcohol consumption. Similar findings have been reported in studies conducted during and during the COVID-19 pandemic, indicating that a decline in financial stability due to the COVID-19 pandemic was associated with higher rates of alcohol consumption among adolescents [8,26]. A study conducted in the United States revealed that negative changes in self-reported financial situations during the COVID-19 pandemic were independently associated with the enhanced likelihood of alcohol consumption (odds ratio, 0.70; p = 0.04) [26]. Moreover, adolescents from families experiencing a decline in income, even outside the pandemic context, were more prone to alcohol consumption. Those from unstable, low-income families were 2.86× more likely to engage in alcohol consumption than their counterparts from families with a stable, adequate income [27]. In addition, the relationship between economic hardship and alcohol use can potentially be mediated by maternal psychological distress and parenting behaviors [28].
- Our study had certain limitations that should be acknowledged. First, it was a cross-sectional study, which means that we were unable to observe changes in students’ behavior and economic status over time. Instead, we relied on a single question asking students to rate the extent of change in their behavior and family economic hardship during the COVID-19 period as compared to before the pandemic. The subjective responses to these questions may differ from the objective degree of change for each item. Further research is needed to determine the extent to which subjective responses to these questions are consistent with objective change. Subjective responses may introduce undifferentiated misclassification, potentially underestimating the true effect. Furthermore, trends in the responses to economic hardship during the COVID-19 pandemic showed substantial variations across grade levels (Supplemental Material 1). Although responses to economic hardship during the COVID-19 pandemic were similar to the distribution of responses in 2021 and 2020 [11], it is important to assess the reliability of adolescents’ responses regarding subjective economic hardship. Additionally, although the KYRBS questionnaire included smoking as a measure of health behaviors, we were unable to utilize it in the study due to the small number of respondents who reported smoking and the significant number of missing values. The number of respondents who reported smoking was extremely low, particularly among girls.
- Notwithstanding these limitations, our study provided valuable insights into the impact of COVID-19 on the health behaviors of adolescents in Korea, specifically in relation to changes in economic status. We discovered that adolescents’ health behaviors were negatively associated with the financial hardships their families experienced during the pandemic. Furthermore, a low subjective family economic status exacerbated these unfavorable changes in health behaviors. Therefore, it is crucial to implement measures that address the economic challenges arising from stressful events like the COVID-19 pandemic and strive to improve the lifestyles of adolescents under such circumstances.
DISCUSSION
Supplemental Materials
Supplementary Material 1.
Supplementary Material 2.
Supplementary Material 3.
Supplementary Material 4.
Supplementary Material 5.
-
Conflict of Interest
The authors have no conflicts of interest associated with the material presented in this paper.
-
Funding
None.
-
Author Contributions
Conceptualization: Park H, Jung-Choi K. Data curation: Kim C, Lee H. Formal analysis: Kim C, Lee H, Jung-Choi K. Funding acquisition: None. Methodology: Park H, Jung-Choi K. Project administration: Park H, Jung-Choi K. Visualization: Kim C, Lee H. Writing – original draft: Kim C, Lee H. Writing – review & editing: Jung-Choi K, Park H.
Notes
Acknowledgements
| Variables |
Boys |
Girls |
||||||
|---|---|---|---|---|---|---|---|---|
| n | Prevalence (%) | Crude1 | Adjusted2,3,4 | n | Prevalence (%) | Crude1 | Adjusted2,3,4 | |
| Increased breakfast skipping | ||||||||
| Total | 22 823 | 13.1 | - | - | 22 085 | 13.6 | - | - |
| COVID-19-related family economic hardship | ||||||||
| None | 6912 | 11.3 | 1.00 (reference) | 1.00 (reference) | 6245 | 12.5 | 1.00 (reference) | 1.00 (reference) |
| Slight | 8977 | 12.4 | 1.13 (1.01, 1.26) | 1.12 (1.01, 1.25) | 9460 | 12.9 | 1.07 (0.96, 1.20) | 1.06 (0.95, 1.19) |
| Moderate | 5657 | 15.1 | 1.43 (1.28, 1.60) | 1.40 (1.25, 1.57) | 5364 | 15.3 | 1.34 (1.19, 1.51) | 1.30 (1.15, 1.48) |
| Severe | 1277 | 19.2 | 1.95 (1.64, 2.32) | 1.85 (1.55, 2.21) | 1016 | 18.1 | 1.68 (1.38, 2.04) | 1.56 (1.27, 1.92) |
| Subjective family economic status | ||||||||
| High | 9394 | 13.2 | 1.00 (reference) | 1.00 (reference) | 8153 | 14.1 | 1.00 (reference) | 1.00 (reference) |
| Middle | 10 910 | 12.5 | 0.99 (0.90, 1.09) | 0.93 (0.85, 1.02) | 11 635 | 12.9 | 0.96 (0.87, 1.05) | 0.88 (0.80, 0.98) |
| Low | 2519 | 15.2 | 1.31 (1.13, 1.51) | 1.05 (0.91, 1.22) | 2297 | 15.2 | 1.22 (1.06, 1.41) | 0.97 (0.83, 1.13) |
| Decreased physical activity | ||||||||
| Total | 22 823 | 43.1 | - | - | 22 085 | 57.3 | - | - |
| COVID-19-related family economic hardship | ||||||||
| None | 6912 | 40.6 | 1.00 (reference) | 1.00 (reference) | 6245 | 54.7 | 1.00 (reference) | 1.00 (reference) |
| Slight | 8977 | 43.2 | 1.11 (1.03, 1.19) | 1.11 (1.03, 1.19) | 9460 | 57.1 | 1.09 (1.02, 1.16) | 1.11 (1.04, 1.18) |
| Moderate | 5657 | 45.0 | 1.19 (1.10, 1.29) | 1.20 (1.11, 1.31) | 5364 | 60.0 | 1.22 (1.13, 1.33) | 1.26 (1.16, 1.37) |
| Severe | 1277 | 47.8 | 1.33 (1.16, 1.52) | 1.37 (1.19, 1.57) | 1016 | 62.1 | 1.33 (1.15, 1.54) | 1.38 (1.19, 1.60) |
| Subjective family economic status | ||||||||
| High | 9394 | 43.6 | 1.00 (reference) | 1.00 (reference) | 8153 | 57.4 | 1.00 (reference) | 1.00 (reference) |
| Middle | 10 910 | 42.6 | 0.95 (0.89, 1.01) | 0.89 (0.84, 0.95) | 11 635 | 56.9 | 0.96 (0.90, 1.03) | 0.92 (0.86, 0.98) |
| Low | 2519 | 43.6 | 0.97 (0.88, 1.08) | 0.84 (0.76, 0.94) | 2297 | 58.8 | 1.02 (0.92, 1.14) | 0.91 (0.81, 1.02) |
| Increased alcohol consumption | ||||||||
| Total | 22 823 | 2.1 | - | - | 22 085 | 1.7 | - | - |
| COVID-19-related family economic hardship | ||||||||
| None | 6912 | 1.8 | 1.00 (reference) | 1.00 (reference) | 6245 | 1.4 | 1.00 (reference) | 1.00 (reference) |
| Slight | 8977 | 1.8 | 0.95 (0.73, 1.23) | 0.91 (0.70, 1.19) | 9460 | 1.4 | 0.95 (0.73, 1.25) | 0.82 (0.62, 1.09) |
| Moderate | 5657 | 2.7 | 1.45 (1.13, 1.87) | 1.26 (0.96, 1.65) | 5364 | 2.0 | 1.33 (0.99, 1.81) | 1.02 (0.71, 1.45) |
| Severe | 1277 | 3.3 | 1.69 (1.15, 2.49) | 1.41 (0.91, 2.20) | 1016 | 3.6 | 2.26 (1.35, 3.76) | 1.41 (0.81, 2.47) |
| Subjective family economic status | ||||||||
| High | 9394 | 1.7 | 1.00 (reference) | 1.00 (reference) | 8153 | 1.5 | 1.00 (reference) | 1.00 (reference) |
| Middle | 10 910 | 2.2 | 1.11 (0.91, 1.36) | 1.10 (0.87, 1.38) | 11 635 | 1.4 | 0.87 (0.65, 1.16) | 0.77 (0.56, 1.05) |
| Low | 2519 | 3.0 | 1.36 (1.00, 1.86) | 1.05 (0.74, 1.51) | 2297 | 3.4 | 1.95 (1.39, 2.74) | 1.43 (0.97, 2.10) |
Values are presented as POR (95% confidence interval).
POR, prevalence odds ratio; COVID-19, coronavirus disease 2019.
1 The crude POR was adjusted for grade.
2 The adjusted POR of increased breakfast skipping was adjusted for grade, residential area, co-residence with parents, subjective health status, depression status, weekday and weekend wake-up times, subjective family economic status, and COVID-19-related family economic hardship.
3 The adjusted POR of decreased physical activity was adjusted for grade, residential area, co-residence with parents, subjective health status, depression status, average smartphone usage time per day, average time spent sitting down per day, subjective family economic status, and COVID-19-related family economic hardship.
4 The adjusted POR of increased alcohol drinking was adjusted for grade, residential area, co-residence with parents, subjective health status, depression status, smoking status, subjective family economic status, and COVID-19-related family economic hardship.
- 1. World Health Organization. WHO COVID-19 dashboard; 2020 [cited 2023 Jun 2]. Available from: https://data.who.int/dashboards/covid19/cases?n = c
- 2. Kim YK, Poncelet JL, Min G, Lee J, Yang Y. COVID-19: systemic risk and response management in the Republic of Korea. Prog Disaster Sci 2021;12: 100200. https://doi.org/10.1016/j.pdisas.2021.100200ArticlePubMedPMC
- 3. Xiang M, Zhang Z, Kuwahara K. Impact of COVID-19 pandemic on children and adolescents’ lifestyle behavior larger than expected. Prog Cardiovasc Dis 2020;63(4):531-532. https://doi.org/10.1016/j.pcad.2020.04.013ArticlePubMedPMC
- 4. Kang DY, Min SH, Park S. The impact of the COVID-19 pandemic on the Korean economy and industry: an interim assessment of one year after the outbreak. KIET Ind Econ Rev 2021;26(5):6-17Article
- 5. Kang S, Seo MY, Kim SH, Park MJ. Changes in lifestyle and obesity during the COVID-19 pandemic in Korean adolescents: based on the Korea Youth Risk Behavior Survey 2019 and 2020. Ann Pediatr Endocrinol Metab 2022;27(4):281-288. https://doi.org/10.6065/apem.2142228.114ArticlePubMedPMC
- 6. Jung YH, Jang BN, Park M, Park EC. Association between family financial decline due to COVID-19 and generalized anxiety disorder among Korean adolescents. J Affect Disord 2022;309: 411-417. https://doi.org/10.1016/j.jad.2022.04.154ArticlePubMedPMC
- 7. Jung YH, Kim SY, Jang SI, Park EC, Shin J, Suh J. Association between the perceived household financial decline due to COVID-19 and smartphone dependency among Korean adolescents. Int J Environ Res Public Health 2022;19(6):3303. https://doi.org/10.3390/ijerph19063303ArticlePubMedPMC
- 8. Park YS, Jung YH, Park EC, Shin J. Association between perceived decline in family income due to COVID-19 and alcohol consumption among Korean adolescents. J Affect Disord 2022;305: 144-150. https://doi.org/10.1016/j.jad.2022.02.051ArticlePubMedPMC
- 9. Kim Y, Choi S, Chun C, Park S, Khang YH, Oh K. Data resource profile: the Korea Youth Risk Behavior Web-based Survey (KYRBS). Int J Epidemiol 2016;45(4):1076-1076e. https://doi.org/10.1093/ije/dyw070ArticlePubMed
- 10. Lundqvist M, Vogel NE, Levin LÅ. Effects of eating breakfast on children and adolescents: a systematic review of potentially relevant outcomes in economic evaluations. Food Nutr Res 2019;63: https://doi.org/10.29219/fnr.v63.1618Article
- 11. Korea Disease Control and Prevention Agency. Korea Youth Risk Behavior Survey statistics [cited 2023 Jul 1]. Available from: https://www.kdca.go.kr/yhs/home.jsp?id = m03_02 (Korean)
- 12. Esquius L, Aguilar-Martínez A, Bosque-Prous M, González-Casals H, Bach-Faig A, Colillas-Malet E, et al. Social inequalities in breakfast consumption among adolescents in Spain: the DESKcohort project. Nutrients 2021;13(8):2500. https://doi.org/10.3390/nu13082500ArticlePubMedPMC
- 13. Kim Y, Yoon J, Kim H, Kwon S. Factors related to eating breakfast of middle and high school students in Seoul. Korean J Community Nutr 2010;15(5):582-592. (Korean)
- 14. Acton RB, Vanderlee L, Cameron AJ, Goodman S, Jáuregui A, Sacks G, et al. Self-reported impacts of the COVID-19 pandemic on diet-related behaviors and food security in 5 countries: results from the International Food Policy Study 2020. J Nutr 2022;152(Suppl 1):35S-46S. https://doi.org/10.1093/jn/nxac025ArticlePubMed
- 15. Young-Hoon KN. A longitudinal study on the impact of income change and poverty on smoking cessation. Can J Public Health 2012;103(3):189-194. https://doi.org/10.1007/BF03403811ArticlePubMedPMC
- 16. Lee DW, Shin J, Choi DW, Kim K, Park EC. Effects of household income change on children’s problem behavior: findings from a longitudinal study. J Adolesc Health 2019;65(4):527-535. https://doi.org/10.1016/j.jadohealth.2019.05.003ArticlePubMed
- 17. Skafida V, Treanor MC. Do changes in objective and subjective family income predict change in children’s diets over time? Unique insights using a longitudinal cohort study and fixed effects analysis. J Epidemiol Community Health 2014;68(6):534-541. https://doi.org/10.1136/jech-2013-203308ArticlePubMed
- 18. Kim NH, Lee JM, Yoo E. How the COVID-19 pandemic has changed adolescent health: physical activity, sleep, obesity, and mental health. Int J Environ Res Public Health 2022;19(15):9224. https://doi.org/10.3390/ijerph19159224ArticlePubMedPMC
- 19. Kwon R, Koo MJ, Lee SW, Choi YS, Shin YH, Shin JU, et al. National trends in physical activity among adolescents in South Korea before and during the COVID-19 pandemic, 2009-2021. J Med Virol 2023;95(2):e28456. https://doi.org/10.1002/jmv.28456ArticlePubMed
- 20. Sampson L, Ettman CK, Abdalla SM, Colyer E, Dukes K, Lane KJ, et al. Financial hardship and health risk behavior during COVID-19 in a large US national sample of women. SSM Popul Health 2021;13: 100734. https://doi.org/10.1016/j.ssmph.2021.100734ArticlePubMedPMC
- 21. Ullrich-French S, McDonough MH. Correlates of long-term participation in a physical activity-based positive youth development program for low-income youth: sustained involvement and psychosocial outcomes. J Adolesc 2013;36(2):279-288. https://doi.org/10.1016/j.adolescence.2012.11.006ArticlePubMed
- 22. Tsang SK, Hui EK, Law BC. Self-efficacy as a positive youth development construct: a conceptual review. ScientificWorldJournal 2012;2012: 452327. https://doi.org/10.1100/2012/452327ArticlePubMedPMC
- 23. Whitbeck LB, Simons RL, Conger RD, Wickrama KA, Ackley KA, Elder Jr GH. The effects of parents’ working conditions and family economic hardship on parenting behaviors and children’s self-efficacy. Soc Psychol Q 1997;60(4):291-303. https://doi.org/10.2307/2787091Article
- 24. Taylor WC, Baranowski T, Young DR. Physical activity interventions in low-income, ethnic minority, and populations with disability. Am J Prev Med 1998;15(4):334-343. https://doi.org/10.1016/s0749-3797(98)00081-6ArticlePubMed
- 25. Oh CM, Kim Y, Yang J, Choi S, Oh K. Changes in health behaviors and obesity of Korean adolescents before and during the COVID-19 pandemic: a special report using the Korea Youth Risk Behavior Survey. Epidemiol Health 2023;45: e2023018. https://doi.org/10.4178/epih.e2023018ArticlePubMedPMC
- 26. Temple JR, Baumler E, Wood L, Guillot-Wright S, Torres E, Thiel M. The impact of the COVID-19 pandemic on adolescent mental health and substance use. J Adolesc Health 2022;71(3):277-284. https://doi.org/10.1016/j.jadohealth.2022.05.025ArticlePubMedPMC
- 27. Poonawalla IB, Kendzor DE, Owen MT, Caughy MO. Family income trajectory during childhood is associated with adolescent cigarette smoking and alcohol use. Addict Behav 2014;39(10):1383-1388. https://doi.org/10.1016/j.addbeh.2014.05.005ArticlePubMedPMC
- 28. Hardaway CR, Cornelius MD. Economic hardship and adolescent problem drinking: family processes as mediating influences. J Youth Adolesc 2014;43: 1191-1202. https://doi.org/10.1007/s10964-013-0063-xArticlePubMed
REFERENCES
Figure & Data
References
Citations
 PubReader
PubReader ePub Link
ePub Link Cite
Cite- Figure
-
- Related articles
-
- Gender Inequalities in Mental Health During the COVID-19 Pandemic: A Population-based Study in Korea
- Associations Between Conventional Healthy Behaviors and Social Distancing During the COVID-19 Pandemic: Evidence From the 2020 Community Health Survey in Korea
- The Impact of Household Economic Deterioration Caused by the COVID-19 Pandemic and Socioeconomic Status on Suicidal Behaviors in Adolescents: A Cross-sectional Study Using 2020 Korea Youth Risk Behavior Web-based Survey Data

