
Articles
- Page Path
- HOME > J Prev Med Public Health > Volume 52(6); 2019 > Article
-
Original Article
Effect of Burnout on Post-traumatic Stress Disorder Symptoms Among Firefighters in Korea: Data From the Firefighter Research on Enhancement of Safety & Health (FRESH) -
Woojin Kim1
 , Munjoo Bae2, Sei-Jin Chang3, Jin-Ha Yoon4, Da Yee Jeong5, Dae-Sung Hyun3,6, Hye-Yoon Ryu7, Ki-Soo Park8, Mi-Ji Kim8, Changsoo Kim1,9
, Munjoo Bae2, Sei-Jin Chang3, Jin-Ha Yoon4, Da Yee Jeong5, Dae-Sung Hyun3,6, Hye-Yoon Ryu7, Ki-Soo Park8, Mi-Ji Kim8, Changsoo Kim1,9 -
Journal of Preventive Medicine and Public Health 2019;52(6):345-354.
DOI: https://doi.org/10.3961/jpmph.19.116
Published online: October 24, 2019
1Department of Preventive Medicine, Yonsei University College of Medicine, Seoul, Korea
2Department of Occupational and Environmental Health, Yonsei University Graduate School of Public Health, Seoul, Korea
3Department of Preventive Medicine and Institute of Occupational and Environmental Medicine, Yonsei University Wonju College of Medicine, Wonju, Korea
4Department of Preventive Medicine and Institute of Occupational Medicine, Yonsei University College of Medicine, Seoul, Korea
5Department of Dental Hygiene, Hanyang Women’s University, Seoul, Korea
6Department of Biostatistics and Computing, Graduate School, Yonsei University, Seoul, Korea
7Department of Preventive Medicine, Yonsei University Wonju College of Medicine, Wonju, Korea
8Department of Preventive Medicine and Institute of Health Science, Gyeongsang National University College of Medicine, Jinju, Korea
9Institute of Human Complexity and Systems Science, Yonsei University, Incheon, Korea
- Corresponding author: Changsoo Kim, MD, PhD Department of Preventive Medicine, Yonsei University College of Medicine, 50 Yonsei-ro, Seodaemun-gu, Seoul 03722, Korea E-mail: preman@yuhs.ac
Copyright © 2019 The Korean Society for Preventive Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
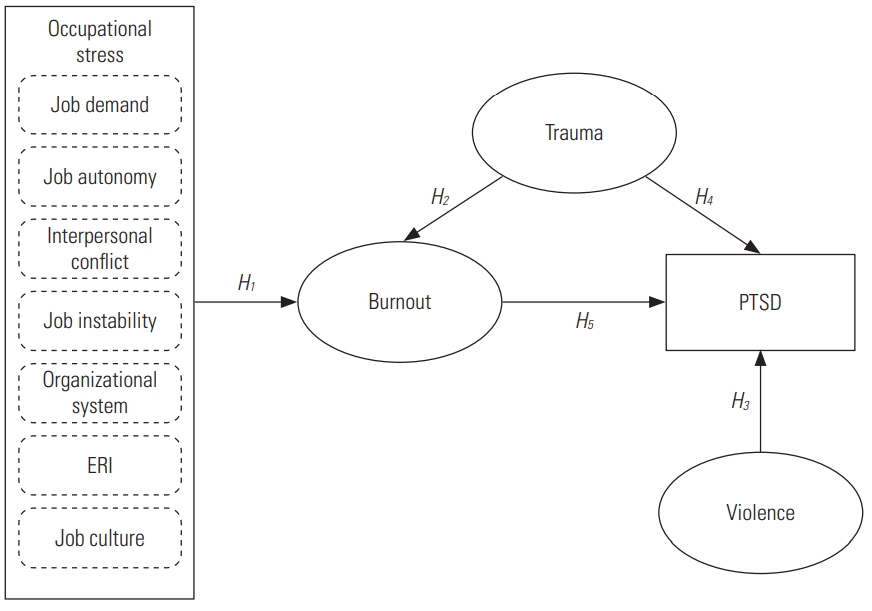

Figure & Data
References
Citations
- Association between burnout and post‐traumatic stress disorder among frontline nurse during COVID‐19 pandemic: A moderated mediation analysis
Leilei Liang, Yuanchao Hu, Junsong Fei, Tongshuang Yuan, Ren Gao, Jingyi Yue, Qianqian Song, Xixi Zhao, Songli Mei
Journal of Clinical Nursing.2024; 33(3): 1076. CrossRef - Post-Traumatic Stress Disorder Symptoms among Pediatric Healthcare Workers
Nikolaos Rigas, Zacharias Kyritsis, Maria Dagla, Alexandra Soldatou, Eirini Orovou, Maria Tzitiridou-Chatzopoulou, Panagiotis Eskitzis, Evangelia Antoniou
Nursing Reports.2024; 14(1): 115. CrossRef - Moderating effect of work fatigue on the association between resilience and posttraumatic stress symptoms: a cross-sectional multi-country study among pharmacists during the COVID-19 pandemic
Samar Younes, Souheil Hallit, Irfan Mohammed, Sarah El Khatib, Anna Brytek-Matera, Shadrach Chinecherem Eze, Kenneth Egwu, Rawshan Jabeen, Nebojša Pavlović, Pascale Salameh, Michelle Cherfane, Marwan Akel, Chadia Haddad, Randa Choueiry, Feten Fekih-Romdha
BioPsychoSocial Medicine.2024;[Epub] CrossRef - Post-traumatic stress disorder in international surgeons undertaking trauma electives in a South African trauma centre
V Thirayan, VY Kong, H Uchino, DL Clarke
South African Journal of Surgery.2024; 62(1): 14. CrossRef - Firefighters and Spouses: Hostility, Satisfaction, and Conflict
Romana Pasca, Shannon L. Wagner
Journal of Family Issues.2023; 44(4): 1074. CrossRef - Psychological Variables Associated With Post-Traumatic Stress Disorder in Firefighters: A Systematic Review
Elena R. Serrano-Ibáñez, Tania Corrás, Mirtha del Prado, Javier Diz, Carmen Varela
Trauma, Violence, & Abuse.2023; 24(4): 2049. CrossRef - Burnout and post-traumatic stress disorder symptoms among medical staff two years after the COVID-19 pandemic in Wuhan, China: Social support and resilience as mediators
Yifang Liu, Li Zou, Shijiao Yan, Pu Zhang, Jun Zhang, Jing Wen, Jing Mao, Longti Li, Ying Wang, Wenning Fu
Journal of Affective Disorders.2023; 321: 126. CrossRef - Compassion Fatigue and Perceived Social Support among Polish Nurses
Paulina Pergol-Metko, Anna Staniszewska, Sebastian Metko, Zofia Sienkiewicz, Lukasz Czyzewski
Healthcare.2023; 11(5): 706. CrossRef - Occupational Stress and Burnout in the Fire Service: Examining the Complex Role and Impact of Sleep Health
Mari-Amanda A. Dyal, Todd D. Smith, David M. DeJoy, Brian A. Moore
Behavior Modification.2022; 46(2): 374. CrossRef - Student Burnout and PTSD Symptoms: The Role of Existential Anxiety and Academic Fears on Students during the COVID 19 Pandemic
Katarzyna Tomaszek, Agnieszka Muchacka-Cymerman, Giovanni Galeoto
Depression Research and Treatment.2022; 2022: 1. CrossRef - The short form effort−reward imbalance: Measure of occupational stress for firefighters
Dal Lae Chin, MinJung Kyung, Jian Li, Stephanie Phelps, OiSaeng Hong
American Journal of Industrial Medicine.2022; 65(6): 492. CrossRef - Emergency nurses' burnout levels as the mediator of the relationship between stress and posttraumatic stress disorder symptoms during COVID‐19 pandemic
Bey‐Jing Yang, Ching‐Wei Yen, Shou‐Ju Lin, Chien‐Hua Huang, Jhong‐Lin Wu, Yih‐Ru Cheng, Chia‐Chen Hsieh, Fei‐Hsiu Hsiao
Journal of Advanced Nursing.2022; 78(9): 2861. CrossRef - Workplace stressors and PTSD among psychiatric workers: The mediating role of burnout
Elke Ham, Michael C. Seto, Nicole C. Rodrigues, N. Zoe Hilton
International Journal of Mental Health Nursing.2022; 31(5): 1151. CrossRef - Testosterone and occupational burnout in professional male firefighters
Denis Vinnikov, Zhanna Romanova, Gulnara Kapanova, Aizhan Raushanova, Sundetgali Kalmakhanov, Alexander Zhigalin
BMC Public Health.2021;[Epub] CrossRef - Doctors and Nurses: A Systematic Review of the Risk and Protective Factors in Workplace Violence and Burnout
Jose Miguel Giménez Lozano, Juan Pedro Martínez Ramón, Francisco Manuel Morales Rodríguez
International Journal of Environmental Research and Public Health.2021; 18(6): 3280. CrossRef - A Relational Model for Stress: A Systematic Review of the Risk and Protective Factors for Stress-Related Diseases in Firefighters
Joana Proença Becker, Rui Paixão, Manuel João Quartilho
Psych.2020; 2(1): 74. CrossRef - PTSD symptoms among health workers and public service providers during the COVID-19 outbreak
Sverre Urnes Johnson, Omid V. Ebrahimi, Asle Hoffart, Kristin Vickers
PLOS ONE.2020; 15(10): e0241032. CrossRef - A Systematic Review and Meta-analysis on the Factors Related to Post-traumatic Growth of Fire Officials
Myung-Gwan Kim, Seung-Woo Han
Journal of Health Informatics and Statistics.2020; 45(4): 373. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite


