Articles
- Page Path
- HOME > J Prev Med Public Health > Volume 45(2); 2012 > Article
-
Original Article
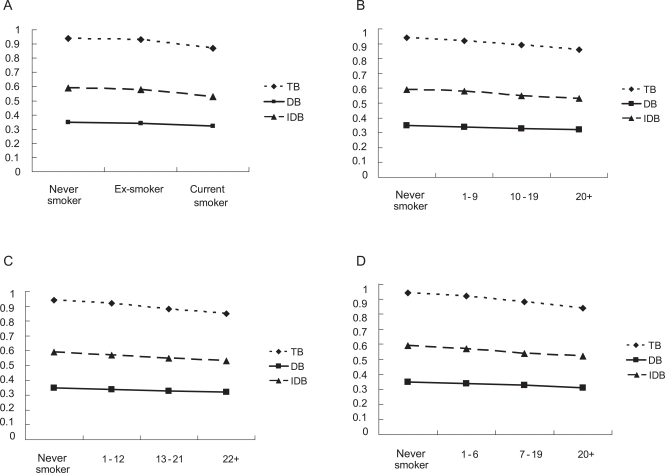
Cigarette Smoking and Serum Bilirubin Subtypes in Healthy Korean Men: The Korea Medical Institute Study - Jaeseong Jo1,2, Heejin Kimm1, Ji Eun Yun1, Kyu Jang Lee3, Sun Ha Jee1
-
Journal of Preventive Medicine and Public Health 2012;45(2):105-112.
DOI: https://doi.org/10.3961/jpmph.2012.45.2.105
Published online: March 31, 2012
1Institute for Health Promotion, Department of Epidemiology and Health Promotion, Yonsei University Graduate School of Public Health, Seoul, Korea.
2Department of Public Health, Yonsei University Graduate School, Seoul, Korea.
3Korea Medical Institute, Seoul, Korea.
- Corresponding author: Sun Ha Jee, MPH, PhD. 50 Yonsei-ro, Seodaemun-gu, Seoul 120-749, Korea. Tel: +82-2-2228-1523, Fax: +82-2-365-5118, jsunha@yuhs.ac
• Received: August 14, 2011 • Accepted: October 17, 2011
Copyright © 2012 The Korean Society for Preventive Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
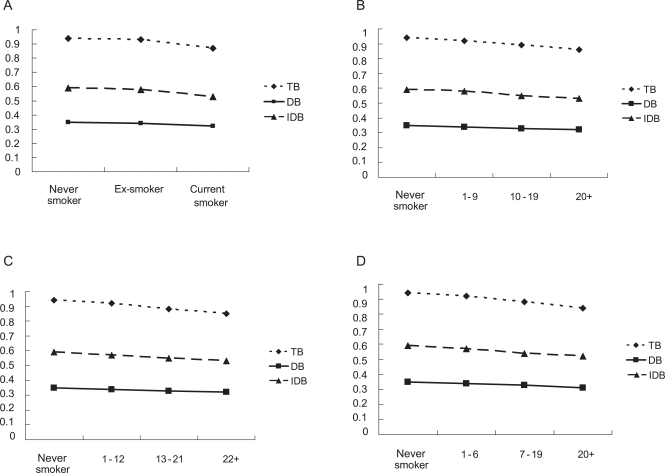
Figure & Data
References
Citations
Citations to this article as recorded by 
- Association between elevated serum bilirubin levels with preserved lung function under conditions of exposure to air pollution
Udi Shapira, Rafael Y. Brezinski, Ori Rogowski, David Zeltser, Shlomo Berliner, Itzhak Shapira, Shani Shenhar-Tsarfaty, Elizabeth Fireman
BMC Pulmonary Medicine.2021;[Epub] CrossRef - ROLE OF BILIRUBIN AS A POTENTIALANTIOXIDANT IN SMOKERS
Varshini. S, A. Preethi, G. Udayakumari
INTERNATIONAL JOURNAL OF SCIENTIFIC RESEARCH.2021; : 43. CrossRef - Direct Bilirubin Levels and Risk of Metabolic Syndrome in Healthy Chinese Men
Xiao-Hong Li, Hai-Yan Lin, Li-Ying Guan, Hui Peng, Meng-Meng Wen, Yong-Qian Cao, Xiu-Yun Jiang, Yi-Bing Wang
BioMed Research International.2017; 2017: 1. CrossRef - Serum bilirubin levels are inversely associated with PAI-1 and fibrinogen in Korean subjects
Hyun Sun Cho, Sung Won Lee, Eun Sook Kim, Juyoung Shin, Sung Dae Moon, Je Ho Han, Bong Yun Cha
Atherosclerosis.2016; 244: 204. CrossRef - Active and Passive Smoking and Serum Total Bilirubin in a Rural Korean Population
Na Hyun Kim, Hyeon Chang Kim, Joo Young Lee, Ju-Mi Lee, Il Suh
Nicotine & Tobacco Research.2016; 18(5): 572. CrossRef - Cigarette smoking behaviour and blood metabolomics
Fangyi Gu, Andriy Derkach, Neal D Freedman, Maria Teresa Landi, Demetrius Albanes, Stephanie J Weinstein, Alison M Mondul, Charles E Matthews, Kristin A Guertin, Qian Xiao, Wei Zheng, Xiao-ou Shu, Joshua N Sampson, Steven C Moore, Neil E Caporaso
International Journal of Epidemiology.2016; 45(5): 1421. CrossRef - Cigarette Smoking Habit and Subjective Quality of Sleep
Alimohamad Asghari, Seyed Kamran Kamrava, Mohsen Rezaee Hemami, Maryam Jalessi, Parin Yazdanifard, Mohammad Farhadi, Seyed Behzad Pousti, Seyed Saleh Tabatabaie
Scimetr.2015;[Epub] CrossRef - Serum Bilirubin Levels Predict Future Development of Metabolic Syndrome in Healthy Middle-aged Nonsmoking Men
Shao-Sung Huang, Wan-Leong Chan, Hsin-Bang Leu, Po-Hsun Huang, Shing-Jong Lin, Jaw-Wen Chen
The American Journal of Medicine.2015; 128(10): 1138.e35. CrossRef - Serum bilirubin concentration is modified by UGT1A1 Haplotypes and influences risk of Type-2 diabetes in the Norfolk Island genetic isolate
M. C. Benton, R. A. Lea, D. Macartney-Coxson, C. Bellis, M. A. Carless, J. E. Curran, M. Hanna, D. Eccles, G. K. Chambers, J. Blangero, L. R. Griffiths
BMC Genetics.2015;[Epub] CrossRef - Serum Bilirubin and Disease Progression in Mild COPD
Scott Apperley, Hye Yun Park, Daniel T. Holmes, S. F. Paul Man, Donald Tashkin, Robert A. Wise, John E. Connett, Don D. Sin
Chest.2015; 148(1): 169. CrossRef - Smoking Cessation Is Followed by Increases in Serum Bilirubin, an Endogenous Antioxidant Associated With Lower Risk of Lung Cancer and Cardiovascular Disease
Stephanie S. O’Malley, Ran Wu, Susan T. Mayne, Peter I. Jatlow
Nicotine & Tobacco Research.2014; 16(8): 1145. CrossRef - Combined Effects of Smoking and Bilirubin Levels on the Risk of Lung Cancer in Korea: The Severance Cohort Study
Jung-eun Lim, Heejin Kimm, Sun Ha Jee, Suminori Akiba
PLoS ONE.2014; 9(8): e103972. CrossRef - The Relationship between Total Bilirubin Levels and Total Mortality in Older Adults: The United States National Health and Nutrition Examination Survey (NHANES) 1999-2004
Kwok-Leung Ong, Matthew A. Allison, Bernard M. Y. Cheung, Ben J. Wu, Philip J. Barter, Kerry-Anne Rye, Shree Ram Singh
PLoS ONE.2014; 9(4): e94479. CrossRef - The Association Between Heterozygosity forUGT1A1*6,UGT1A1*28, and Variation in the Serum Total-Bilirubin Level in Healthy Young Japanese Adults
Hiroyuki Moriya, Katsuhiko Saito, Nuala Helsby, Shigekazu Sugino, Michiaki Yamakage, Masahiko Takasaki, Hidenori Kato, Nahoko Kurosawa
Genetic Testing and Molecular Biomarkers.2013; 17(6): 464. CrossRef - Serum bilirubin may serve as a marker for increased heme oxygenase activity and inducibility in tissues – A rationale for the versatile health protection associated with elevated plasma bilirubin
Mark F. McCarty
Medical Hypotheses.2013; 81(4): 607. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite