Cigarette Smoking and Serum Bilirubin Subtypes in Healthy Korean Men: The Korea Medical Institute Study
Article information
Abstract
Objectives
Cigarette smoking is a modifiable risk factor for cardiovascular disease. Bilirubin is a potent antioxidant and its concentration decreases in smokers. However, studies about the association between cigarette smoking and bilirubin are scarce and most are limited to total bilirubin. Additionally, bilirubin is highly related to hemoglobin. Therefore, this study evaluates the association between bilirubin subtypes and cigarette smoking in healthy Korean men independently of hemoglobin.
Methods
This study included 48 040 Korean men aged 30 to 87 years who visited the Korea Medical Institute for routine health examinations from January to December, 2007. The association of smoking with total, direct, and indirect bilirubin was assessed by logistic regression analysis taking into consideration differences in subjects and smoking characteristics.
Results
Current smokers had lower bilirubin concentrations than never-smokers and ex-smokers. Smoking amount and duration were inversely significantly associated with total, direct, and indirect bilirubin. In a multivariable adjusted model, compared to never-smokers, the odds ratios (ORs) and 95% confidence intervals (CIs) of current smokers with the highest number of pack-years were 1.7 (1.6 to 1.9) for total, 1.5 (1.4 to 1.6) for direct, and 1.7 (1.6 to 1.9) for indirect bilirubin. After further adjustment for hemoglobin, this association became stronger (OR [95% CI], 2.1 [1.9 to 2.2] for total; 1.9 [1.8 to 2.0] for direct; 2.0 [1.9 to 2.2] for indirect bilirubin).
Conclusions
In this study, bilirubin subtypes are inversely associated with smoking status, smoking amount, and smoking duration in healthy Korean men independently of hemoglobin. Further studies are needed to investigate this association in healthy Korean women.
INTRODUCTION
Cigarette smoking is a major modifiable risk factor for cardiovascular disease (CVD) [1]. Cigarette smoking accounts for approximately 400 million deaths each year worldwide. Reportedly, about 70% of smoking deaths have taken place in Asian countries [2]. Cigarette smoking is considered to be the first leading preventable cause of death in Korean men. According to the fourth Korean National Health and Nutrition Examination Survey in 2007, of persons 20 years or older, the smoking rate in South Korea was 50.8% for men and 3.2% for women [3].
Serum bilirubin, which is a bile pigment, is known as a major breakdown product of heme catabolism and thus is highly related to hemoglobin [4]. Bilirubin circulates in the bloodstream in two forms: direct and indirect. It has been found to have potent endogenous antioxidant properties in in vitro studies, whether in direct or indirect form. It protects lipid membranes, protein albumin, and other proteins, especially in areas consisting of poor antioxidant defense systems such as the myocardium and nervous system [5,6]. Bilirubin concentrations were found to have inverse associations with the risk of CVD, stroke, and metabolic syndrome [7-9]. The serum bilirubin subtypes, especially direct bilirubin, have also been found to have significant associations with metabolic syndrome components including central obesity, hypertriglyceridemia, hyperglycemia, and low levels of high-density lipoprotein cholesterol (HDL-C) for both genders [10]. Still, studies identifying the impact of serum bilirubin subtypes on the risk of CVD, stroke, and metabolic syndrome are scarce.
An association between cigarette smoking and serum bilirubin has been suggested by some studies. In these studies, smoking was associated with decreased serum bilirubin concentrations [11-14]. However, smoking was also found to have a significant association with hemoglobin, which regulates bilirubin concentrations [15,16]. Whether smoking can be affected by hemoglobin in relation to bilirubin is still questionable. Moreover, most of the previous data on cigarette smoking in relation to serum bilirubin has been limited to total bilirubin. Therefore, we evaluated the association between bilirubin subtypes and cigarette smoking status, smoking intensity, and duration of current smoking in healthy Korean men independently of hemoglobin levels.
METHODS
I. Study Subjects
This study included 55 183 Korean men aged 30 to 89 years who visited the Korea Medical Institute (KMI) from January, 2007 to December, 2007. Of the 55 183 participants, 551 aged <30 years were excluded for having missing data for bilirubin subtypes: total, direct, and indirect bilirubin. Another 734 were excluded for having missing data for systolic blood pressure, diastolic blood pressure, waist circumference, triglycerides, fasting serum glucose, and alcohol consumption. Participants with total bilirubin >34.2 µol/L (2 mg/dL) were excluded due to a high possibility of Gilbert's syndrome [9]. Furthermore, 119 participants with a past history of CVD and liver diseases identified in the self-questionnaire and 337 who had a history of cancer, CVD, stroke, diabetes, or hypertension were also excluded. Therefore, the study population was finalized as 48 040 Korean men. Recruitment of volunteers only took place after obtaining written informed consent. The Institutional Review Board of Human Research of Yonsei University approved the study.
II. Data Collection
During a standardized examination at KMI, participants were asked whether they had ever smoked or whether they exercised regularly via a standardized health questionnaire. Demographic characteristics including age, gender, family history, and past history of clinical diseases, as well as cigarette smoking status (never-smoker, ex-smoker, or current-smoker) and alcohol consumption status (never-drinker and ever-drinker) were also collected. Both current- and ex-smokers were asked to report the average number of cigarettes per day they smoked at the time or had smoked earlier. Waist circumference was measured midway between the lower rib and iliac crest. Pack-years (PYR) were calculated as follows: PYR=smoking amount (cigarettes/d)×period of smoking (y)/20.
For clinical chemistry assays, serum was separated from peripheral venous blood samples obtained from each participant after 12 hours of fasting. Serum bilirubin, fasting blood glucose, total cholesterol, triglycerides, and HDL-C were measured using a Hitachi-7600 analyzer (Hitachi Ltd., Tokyo, Japan). The body mass index (BMI) was calculated as weight (kg) divided by the square of height (m2).
III. Statistical Analysis
Data were expressed as mean±standard deviation. ANOVA was used to analyze statistical differences among the characteristics of the study participants. Current-smokers were classified into groups smoking 1 to 9, 10 to 19, and 20 or more cigarettes per day. Smokers were further classified into groups by duration of smoking of 1 to 12, 13 to 21, and 22 or more years. Multiple logistic regression analysis was employed to identify the association between cigarette smoking and serum bilirubin subtypes in current smokers. To examine the association between smoking status and total serum bilirubin, stratified by age, BMI, hypertension, diabetes, triglyceride (TG)/HDL-C, and alcohol intake, samples were divided into groups by median value of age (<40 and ≥40), BMI (<23 and ≥23), hypertension (yes and no), diabetes (yes and no), TG/HDL-C (<3 and ≥3) and alcohol intake (yes and no). Hypobilirubinemia was defined as the lowest quartile of bilirubin subtypes [17].
All analysis was conducted using SAS version 9.1 (SAS Institute Inc., Cary, NC, USA). All statistical tests were two-sided and statistical significance was determined as p<0.05.
RESULTS
Table 1 shows the general characteristics of Korean men (n=48 040) in relation to smoking status. The percentages of participants aged 30 to 89 years classified as never-smokers, ex-smokers, and current-smokers were 31.2%, 23.0%, and 45.8%, respectively. Never-smokers were younger, on average, than ex-smokers and older than current-smokers. Compared to never-smokers, ex-smokers and current-smokers had a larger average waist circumference, and higher levels of total cholesterol, triglycerides, alanine aminotransferase (ALT), and gamma-glutamyl transferase (GGT). However, HDL-C and serum bilirubin subtype levels were lower in ex-smokers and current-smokers than never-smokers. All of these differences were statistically significant (p<0.05). Mean total serum bilirubin concentrations were 14.8 µol/L and 16.1 µol/L in current-smokers and never-smokers, respectively. Additionally, mean concentrations of total, direct, and indirect serum bilirubin decreased with increasing numbers of cigarettes smoked per day, period of smoking, and PYR in current-smokers (Figure 1).

General characteristics of Korean men according to smoking status
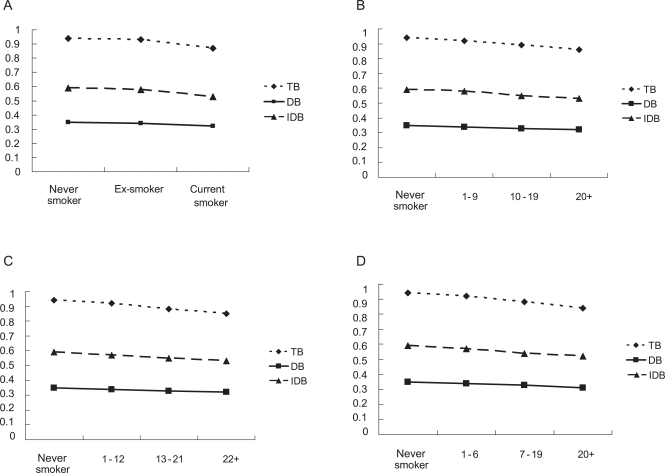
Means of total, direct and indirect serum bilirubin versus cigarette smoking among Korean men (p for trend < 0.01). (A) Smoking status. (B) smoking amount (cigarettes/d) in current smokers. (C) Smoking duration (y) in current smokers. (D) Pack-years in current smokers.
TB, total bilirubin; DB, direct bilirubin; IDB, indirect bilirubin.
Table 2 details the multiple logistic regression model of the lowest quartile of serum bilirubin subtypes compared to the highest quartile in current-smokers among men. After adjusting for age, BMI, ALT, GGT, uric acid, and alcohol consumption in model I, serum bilirubin subtypes, including total, direct, and indirect bilirubin, were inversely significantly associated with smoking amount, smoking duration, and PYR. When hemoglobin was further adjusted in model II, these associations of serum bilirubin subtypes with smoking amount and PYR remained statistically significant and were even stronger. However, the association between serum bilirubin subtypes and smoking duration remained the same after further adjusting for hemoglobin. In model I, compared to never smokers, the odds ratios (ORs) and 95% confidence intervals (CI) of current smokers with PYR ≥20 years for the lowest quartile of serum bilirubin subtypes were 1.7 (1.6-1.9) for total, 1.5 (1.4-1.6) for direct, and 1.7 (1.6-1.9) for indirect bilirubin whereas the ORs (95% CI) of current smokers with pack-years ≥20 years, compared to never smokers, for the lowest quartile of serum bilirubin subtypes increased to 2.1 (1.9-2.2) for total, 1.9 (1.8-2.0) for direct, and 2.0 (1.9-2.2) for indirect bilirubin in model II.
Current smokers were grouped according to the quantity of cigarettes smoked per day (0, 1-9, 10-19, and 20 or more) in order to examine the association between smoking intensity and total serum bilirubin concentration. The data were further stratified by age, BMI, hypertension, diabetes, TG/HDL-C ratio, and alcohol intake (Table 3). Compared to never-smokers, ORs (95% CI) for the lowest quartile of total bilirubin increased in men who smoked more than 20 cigarettes per day to 1.6 (1.4-1.7) and 1.6 (1.5-1.7), with age <40 and age ≥40 years, respectively. In addition, men who drank and smoked more than 20 cigarettes per day had an OR (95% CI) of 1.6 (1.5-1.7) whereas men who did not drink and smoke more than 20 cigarettes per day had an OR (95% CI) of 1.9 (1.7-2.2). Similar relationships between total serum bilirubin and smoking intensity were seen in BMI, hypertension, diabetes, and TG/HDL-C ratios.

ORs and 95% CIs for the lowest quartile of total bilirubin concentration compared to the highest quartile of total bilirubin concentrations according to age, BMI, hypertension, diabetes, TG/HDL-C, and alcohol intake in current male smokers
DISCUSSION
Our study demonstrated that cigarette smoking is associated with lower concentrations of serum bilirubin among healthy Korean men. Lower concentrations of serum bilirubin subtypes, including total, direct, and indirect, were found in ex- and current smokers than never smokers. Additionally, concentrations of serum bilirubin subtypes decreased with increasing numbers of cigarettes smoked per day, period of smoking, and PYR among current-smokers. In this study, these significant associations were independent of hemoglobin levels.
Cigarette smoking is known to be a modifiable risk factor for CVD and the leading cause of death in Korea. The association between cigarette smoking and serum bilirubin concentration has been described previously [11-14]. In a study among the Belgian population, total serum bilirubin concentration was lower in male smokers and intermediate in former-smokers compared with never-smokers. Although lower concentrations of total serum bilirubin were found in female smokers, the difference was not significant [14]. In a study among US residents, a significant inverse association between smoking and total serum bilirubin was found. In particular, this inverse association occurred in subjects without coronary artery disease (CAD) and subjects with minimal CAD and severe CAD [13]. Although inverse associations between total serum bilirubin and smoking status were reported in these studies, the importance of bilirubin as an antioxidant affected by smoking needs further investigation. However, cigarette smoking is also found to be positively associated with hemoglobin, which regulates bilirubin concentrations [15,16]. Therefore, differences in bilirubin levels may be due to hemoglobin concentrations. Still, these studies showing the significant associations between total serum bilirubin and smoking were independent of hemoglobin.
Regarding the relationship between smoking and bilirubin subtypes, total, direct, and indirect bilirubin have been consistently shown to be lower in current-smokers than never-smokers. In a study examining the relationship of serum bilirubin subtypes with ischemic stroke, those with higher levels of direct bilirubin had more acute severe stroke than those with lower levels of direct serum bilirubin. Direct serum bilirubin was significantly associated with initial stroke severity, whereas total bilirubin was not. It is still unclear why serum bilirubin, especially direct bilirubin, was significantly associated with initial stroke [18]. In addition, in the relationship of direct bilirubin to metabolic syndrome analyzed in a recent study, the highest quartile of serum direct bilirubin was associated with a 40% to 70% reduced risk of metabolic syndrome relative to the lowest quartile in both men and women. Furthermore, women of the top quartile of serum total bilirubin and serum indirect bilirubin had a 35% and 20% lower rate of the metabolic syndrome, respectively [19]. Some studies indicated that direct bilirubin might act on the target organ and molecule because direct bilirubin is weakly bound to albumin, thus easily separated from albumin and converted into active form than the other bilirubin subtypes [20]. Still, a variety of epidemiological studies among individuals with general medical conditions including hepatic disease have suggested that the direct bilirubin concentration may have a better prognostic value than total bilirubin concentration [18-23]. However, in our study, direct bilirubin together with total and indirect serum bilirubin was significantly associated with smoking among Korean men. Furthermore, total, direct, and indirect serum bilirubin subtypes decreased with increasing smoking amount and duration. From a recent study, the duration of smoking was found to be a more important determinant of serum bilirubin concentration than the number of cigarettes smoked per day [14]. However, in that study, smoking duration was an important determinant of serum bilirubin concentration together with smoking amount.
In this study, an increased risk of having total bilirubin in the lowest quartile was obtained with increasing numbers of cigarettes smoked per day among current smokers in the strata of age, BMI, hypertension, diabetes, TG/HDL-C, and alcohol intake. In particular, these associations were statistically stronger in men who smoked more than 20 cigarettes per day and had a BMI <23 kg/m2, hypertension, diabetes, or TG/HDL-C <3, or who did not drink alcohol.
Bilirubin, which is a bile pigment, is generally regarded as a waste product of heme catabolism. However, it has been suggested that bilirubin might play an important role as an antioxidant, and its role as an antioxidant in vitro has recently been identified [24-28]. A number of recent in vitro studies have shown that bilirubin is more efficient than α-tocopherol at inhibiting low-density lipoprotein (LDL) oxidation and is a more efficient protector of human ventricular myocytes than either vitamin C or vitamin E [29-32]. Cigarette smoke contains a large quantity of free radicals, resulting in endothelial injury [33]. LDL oxidation appears as an early event of atherosclerosis and increases with cigarette smoking [34-36]. In this study, low serum bilirubin levels could have been caused by overconsumption of free-radicals produced mostly by cigarette smoking.
This study has several limitations. Due to its cross-sectional design, the present study precluded the determination of causality. Bilirubin concentrations were measured only once. Another limitation may be that this study was performed only among men due to the small number of female Korean smokers. However, the main strength of this study is that to our knowledge it is a large sample size used to evaluate the inverse association between bilirubin concentration and cigarette smoking among Korean men. Most published studies have been limited to Caucasians rather than Asians. Second, Gilbert's syndrome is a genetic disorder of bilirubin metabolism that can result in production of elevated levels of indirect bilirubin in the bloodstream without any serious consequences [37]. In Korea, participants with Gilbert's syndrome have been shown to have a low prevalence and incidence of coronary heart diseases and higher levels of high density lipoprotein and antioxidant levels [38]. In this study, to clarify the results, only apparently healthy Korean men without a high possibility of having Gilbert's syndrome (total bilirubin concentrations >34.2 µol/L) [9] or any other diseases, which might affect the association between serum bilirubin and smoking, were included in the study. Still, total bilirubin concentrations >34.2 µol/L is not the definition or exclusion of Gilbert's syndrome. We also could not find any differences in the risk of having hypobilirubinemia when we included the participants with Gilbert's syndrome. The association between serum bilirubin and smoking remained significant after the exclusions. Finally, participants in the KMI study were mostly workers; therefore, they were mostly younger than those in the Korean National Health and Nutrition Examination Survey data.
In conclusion, cigarette smoking decreases all three types of serum bilirubin in apparently health Korean men independently of hemoglobin. Bilirubin is inexpensive and easily measured in most clinical laboratories. Further studies are needed to determine if measuring bilirubin is effective in detecting free-radicals produced by smoking, which contribute to serious diseases including CVD. Additionally, further investigations should be carried out to determine whether such associations also exist among apparently healthy Korean women.
ACKNOWLEDGEMENTS
We thank the staff of the Korea Medical Institute (KMI). This study was supported by a grant of the Seoul R&BD program, Republic of Korea (10526), the National R&D Program for Cancer Control, Ministry for Health, Welfare and Family affairs, Republic of Korea (0920330), and the National Research Foundation of Korea grant funded by the Korea government (MEST) (no. 2011-0029348).
Notes
The authors have no conflicts of interest with the material presented in this paper.
This article is available at http://jpmph.org/.