Articles
- Page Path
- HOME > J Prev Med Public Health > Volume 45(2); 2012 > Article
-
Original Article
Cigarette Smoking and Serum Bilirubin Subtypes in Healthy Korean Men: The Korea Medical Institute Study - Jaeseong Jo1,2, Heejin Kimm1, Ji Eun Yun1, Kyu Jang Lee3, Sun Ha Jee1
-
Journal of Preventive Medicine and Public Health 2012;45(2):105-112.
DOI: https://doi.org/10.3961/jpmph.2012.45.2.105
Published online: March 31, 2012
1Institute for Health Promotion, Department of Epidemiology and Health Promotion, Yonsei University Graduate School of Public Health, Seoul, Korea.
2Department of Public Health, Yonsei University Graduate School, Seoul, Korea.
3Korea Medical Institute, Seoul, Korea.
- Corresponding author: Sun Ha Jee, MPH, PhD. 50 Yonsei-ro, Seodaemun-gu, Seoul 120-749, Korea. Tel: +82-2-2228-1523, Fax: +82-2-365-5118, jsunha@yuhs.ac
Copyright © 2012 The Korean Society for Preventive Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Objectives
- Cigarette smoking is a modifiable risk factor for cardiovascular disease. Bilirubin is a potent antioxidant and its concentration decreases in smokers. However, studies about the association between cigarette smoking and bilirubin are scarce and most are limited to total bilirubin. Additionally, bilirubin is highly related to hemoglobin. Therefore, this study evaluates the association between bilirubin subtypes and cigarette smoking in healthy Korean men independently of hemoglobin.
-
Methods
- This study included 48 040 Korean men aged 30 to 87 years who visited the Korea Medical Institute for routine health examinations from January to December, 2007. The association of smoking with total, direct, and indirect bilirubin was assessed by logistic regression analysis taking into consideration differences in subjects and smoking characteristics.
-
Results
- Current smokers had lower bilirubin concentrations than never-smokers and ex-smokers. Smoking amount and duration were inversely significantly associated with total, direct, and indirect bilirubin. In a multivariable adjusted model, compared to never-smokers, the odds ratios (ORs) and 95% confidence intervals (CIs) of current smokers with the highest number of pack-years were 1.7 (1.6 to 1.9) for total, 1.5 (1.4 to 1.6) for direct, and 1.7 (1.6 to 1.9) for indirect bilirubin. After further adjustment for hemoglobin, this association became stronger (OR [95% CI], 2.1 [1.9 to 2.2] for total; 1.9 [1.8 to 2.0] for direct; 2.0 [1.9 to 2.2] for indirect bilirubin).
-
Conclusions
- In this study, bilirubin subtypes are inversely associated with smoking status, smoking amount, and smoking duration in healthy Korean men independently of hemoglobin. Further studies are needed to investigate this association in healthy Korean women.
- Cigarette smoking is a major modifiable risk factor for cardiovascular disease (CVD) [1]. Cigarette smoking accounts for approximately 400 million deaths each year worldwide. Reportedly, about 70% of smoking deaths have taken place in Asian countries [2]. Cigarette smoking is considered to be the first leading preventable cause of death in Korean men. According to the fourth Korean National Health and Nutrition Examination Survey in 2007, of persons 20 years or older, the smoking rate in South Korea was 50.8% for men and 3.2% for women [3].
- Serum bilirubin, which is a bile pigment, is known as a major breakdown product of heme catabolism and thus is highly related to hemoglobin [4]. Bilirubin circulates in the bloodstream in two forms: direct and indirect. It has been found to have potent endogenous antioxidant properties in in vitro studies, whether in direct or indirect form. It protects lipid membranes, protein albumin, and other proteins, especially in areas consisting of poor antioxidant defense systems such as the myocardium and nervous system [5,6]. Bilirubin concentrations were found to have inverse associations with the risk of CVD, stroke, and metabolic syndrome [7-9]. The serum bilirubin subtypes, especially direct bilirubin, have also been found to have significant associations with metabolic syndrome components including central obesity, hypertriglyceridemia, hyperglycemia, and low levels of high-density lipoprotein cholesterol (HDL-C) for both genders [10]. Still, studies identifying the impact of serum bilirubin subtypes on the risk of CVD, stroke, and metabolic syndrome are scarce.
- An association between cigarette smoking and serum bilirubin has been suggested by some studies. In these studies, smoking was associated with decreased serum bilirubin concentrations [11-14]. However, smoking was also found to have a significant association with hemoglobin, which regulates bilirubin concentrations [15,16]. Whether smoking can be affected by hemoglobin in relation to bilirubin is still questionable. Moreover, most of the previous data on cigarette smoking in relation to serum bilirubin has been limited to total bilirubin. Therefore, we evaluated the association between bilirubin subtypes and cigarette smoking status, smoking intensity, and duration of current smoking in healthy Korean men independently of hemoglobin levels.
INTRODUCTION
- I. Study Subjects
- This study included 55 183 Korean men aged 30 to 89 years who visited the Korea Medical Institute (KMI) from January, 2007 to December, 2007. Of the 55 183 participants, 551 aged <30 years were excluded for having missing data for bilirubin subtypes: total, direct, and indirect bilirubin. Another 734 were excluded for having missing data for systolic blood pressure, diastolic blood pressure, waist circumference, triglycerides, fasting serum glucose, and alcohol consumption. Participants with total bilirubin >34.2 µol/L (2 mg/dL) were excluded due to a high possibility of Gilbert's syndrome [9]. Furthermore, 119 participants with a past history of CVD and liver diseases identified in the self-questionnaire and 337 who had a history of cancer, CVD, stroke, diabetes, or hypertension were also excluded. Therefore, the study population was finalized as 48 040 Korean men. Recruitment of volunteers only took place after obtaining written informed consent. The Institutional Review Board of Human Research of Yonsei University approved the study.
- II. Data Collection
- During a standardized examination at KMI, participants were asked whether they had ever smoked or whether they exercised regularly via a standardized health questionnaire. Demographic characteristics including age, gender, family history, and past history of clinical diseases, as well as cigarette smoking status (never-smoker, ex-smoker, or current-smoker) and alcohol consumption status (never-drinker and ever-drinker) were also collected. Both current- and ex-smokers were asked to report the average number of cigarettes per day they smoked at the time or had smoked earlier. Waist circumference was measured midway between the lower rib and iliac crest. Pack-years (PYR) were calculated as follows: PYR=smoking amount (cigarettes/d)×period of smoking (y)/20.
- For clinical chemistry assays, serum was separated from peripheral venous blood samples obtained from each participant after 12 hours of fasting. Serum bilirubin, fasting blood glucose, total cholesterol, triglycerides, and HDL-C were measured using a Hitachi-7600 analyzer (Hitachi Ltd., Tokyo, Japan). The body mass index (BMI) was calculated as weight (kg) divided by the square of height (m2).
- III. Statistical Analysis
- Data were expressed as mean±standard deviation. ANOVA was used to analyze statistical differences among the characteristics of the study participants. Current-smokers were classified into groups smoking 1 to 9, 10 to 19, and 20 or more cigarettes per day. Smokers were further classified into groups by duration of smoking of 1 to 12, 13 to 21, and 22 or more years. Multiple logistic regression analysis was employed to identify the association between cigarette smoking and serum bilirubin subtypes in current smokers. To examine the association between smoking status and total serum bilirubin, stratified by age, BMI, hypertension, diabetes, triglyceride (TG)/HDL-C, and alcohol intake, samples were divided into groups by median value of age (<40 and ≥40), BMI (<23 and ≥23), hypertension (yes and no), diabetes (yes and no), TG/HDL-C (<3 and ≥3) and alcohol intake (yes and no). Hypobilirubinemia was defined as the lowest quartile of bilirubin subtypes [17].
- All analysis was conducted using SAS version 9.1 (SAS Institute Inc., Cary, NC, USA). All statistical tests were two-sided and statistical significance was determined as p<0.05.
METHODS
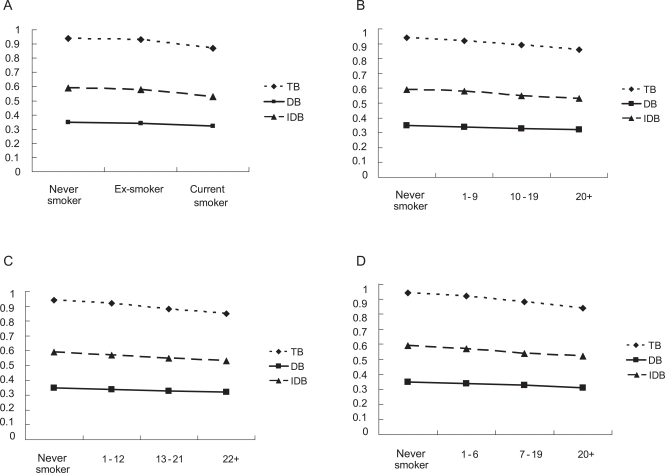
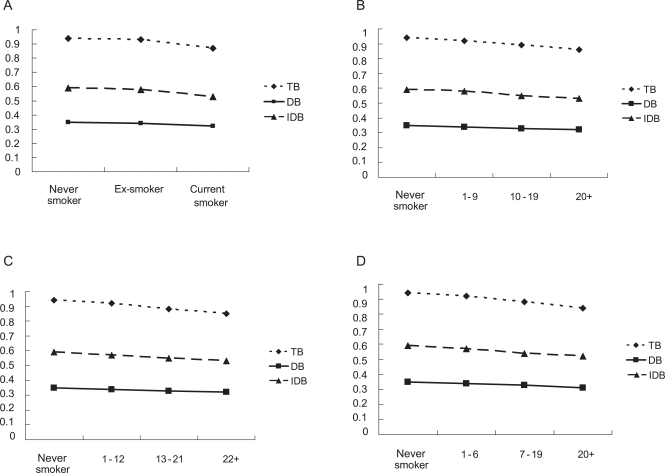
- Table 1 shows the general characteristics of Korean men (n=48 040) in relation to smoking status. The percentages of participants aged 30 to 89 years classified as never-smokers, ex-smokers, and current-smokers were 31.2%, 23.0%, and 45.8%, respectively. Never-smokers were younger, on average, than ex-smokers and older than current-smokers. Compared to never-smokers, ex-smokers and current-smokers had a larger average waist circumference, and higher levels of total cholesterol, triglycerides, alanine aminotransferase (ALT), and gamma-glutamyl transferase (GGT). However, HDL-C and serum bilirubin subtype levels were lower in ex-smokers and current-smokers than never-smokers. All of these differences were statistically significant (p<0.05). Mean total serum bilirubin concentrations were 14.8 µol/L and 16.1 µol/L in current-smokers and never-smokers, respectively. Additionally, mean concentrations of total, direct, and indirect serum bilirubin decreased with increasing numbers of cigarettes smoked per day, period of smoking, and PYR in current-smokers (Figure 1).
- Table 2 details the multiple logistic regression model of the lowest quartile of serum bilirubin subtypes compared to the highest quartile in current-smokers among men. After adjusting for age, BMI, ALT, GGT, uric acid, and alcohol consumption in model I, serum bilirubin subtypes, including total, direct, and indirect bilirubin, were inversely significantly associated with smoking amount, smoking duration, and PYR. When hemoglobin was further adjusted in model II, these associations of serum bilirubin subtypes with smoking amount and PYR remained statistically significant and were even stronger. However, the association between serum bilirubin subtypes and smoking duration remained the same after further adjusting for hemoglobin. In model I, compared to never smokers, the odds ratios (ORs) and 95% confidence intervals (CI) of current smokers with PYR ≥20 years for the lowest quartile of serum bilirubin subtypes were 1.7 (1.6-1.9) for total, 1.5 (1.4-1.6) for direct, and 1.7 (1.6-1.9) for indirect bilirubin whereas the ORs (95% CI) of current smokers with pack-years ≥20 years, compared to never smokers, for the lowest quartile of serum bilirubin subtypes increased to 2.1 (1.9-2.2) for total, 1.9 (1.8-2.0) for direct, and 2.0 (1.9-2.2) for indirect bilirubin in model II.
- Current smokers were grouped according to the quantity of cigarettes smoked per day (0, 1-9, 10-19, and 20 or more) in order to examine the association between smoking intensity and total serum bilirubin concentration. The data were further stratified by age, BMI, hypertension, diabetes, TG/HDL-C ratio, and alcohol intake (Table 3). Compared to never-smokers, ORs (95% CI) for the lowest quartile of total bilirubin increased in men who smoked more than 20 cigarettes per day to 1.6 (1.4-1.7) and 1.6 (1.5-1.7), with age <40 and age ≥40 years, respectively. In addition, men who drank and smoked more than 20 cigarettes per day had an OR (95% CI) of 1.6 (1.5-1.7) whereas men who did not drink and smoke more than 20 cigarettes per day had an OR (95% CI) of 1.9 (1.7-2.2). Similar relationships between total serum bilirubin and smoking intensity were seen in BMI, hypertension, diabetes, and TG/HDL-C ratios.
RESULTS
- Our study demonstrated that cigarette smoking is associated with lower concentrations of serum bilirubin among healthy Korean men. Lower concentrations of serum bilirubin subtypes, including total, direct, and indirect, were found in ex- and current smokers than never smokers. Additionally, concentrations of serum bilirubin subtypes decreased with increasing numbers of cigarettes smoked per day, period of smoking, and PYR among current-smokers. In this study, these significant associations were independent of hemoglobin levels.
- Cigarette smoking is known to be a modifiable risk factor for CVD and the leading cause of death in Korea. The association between cigarette smoking and serum bilirubin concentration has been described previously [11-14]. In a study among the Belgian population, total serum bilirubin concentration was lower in male smokers and intermediate in former-smokers compared with never-smokers. Although lower concentrations of total serum bilirubin were found in female smokers, the difference was not significant [14]. In a study among US residents, a significant inverse association between smoking and total serum bilirubin was found. In particular, this inverse association occurred in subjects without coronary artery disease (CAD) and subjects with minimal CAD and severe CAD [13]. Although inverse associations between total serum bilirubin and smoking status were reported in these studies, the importance of bilirubin as an antioxidant affected by smoking needs further investigation. However, cigarette smoking is also found to be positively associated with hemoglobin, which regulates bilirubin concentrations [15,16]. Therefore, differences in bilirubin levels may be due to hemoglobin concentrations. Still, these studies showing the significant associations between total serum bilirubin and smoking were independent of hemoglobin.
- Regarding the relationship between smoking and bilirubin subtypes, total, direct, and indirect bilirubin have been consistently shown to be lower in current-smokers than never-smokers. In a study examining the relationship of serum bilirubin subtypes with ischemic stroke, those with higher levels of direct bilirubin had more acute severe stroke than those with lower levels of direct serum bilirubin. Direct serum bilirubin was significantly associated with initial stroke severity, whereas total bilirubin was not. It is still unclear why serum bilirubin, especially direct bilirubin, was significantly associated with initial stroke [18]. In addition, in the relationship of direct bilirubin to metabolic syndrome analyzed in a recent study, the highest quartile of serum direct bilirubin was associated with a 40% to 70% reduced risk of metabolic syndrome relative to the lowest quartile in both men and women. Furthermore, women of the top quartile of serum total bilirubin and serum indirect bilirubin had a 35% and 20% lower rate of the metabolic syndrome, respectively [19]. Some studies indicated that direct bilirubin might act on the target organ and molecule because direct bilirubin is weakly bound to albumin, thus easily separated from albumin and converted into active form than the other bilirubin subtypes [20]. Still, a variety of epidemiological studies among individuals with general medical conditions including hepatic disease have suggested that the direct bilirubin concentration may have a better prognostic value than total bilirubin concentration [18-23]. However, in our study, direct bilirubin together with total and indirect serum bilirubin was significantly associated with smoking among Korean men. Furthermore, total, direct, and indirect serum bilirubin subtypes decreased with increasing smoking amount and duration. From a recent study, the duration of smoking was found to be a more important determinant of serum bilirubin concentration than the number of cigarettes smoked per day [14]. However, in that study, smoking duration was an important determinant of serum bilirubin concentration together with smoking amount.
- In this study, an increased risk of having total bilirubin in the lowest quartile was obtained with increasing numbers of cigarettes smoked per day among current smokers in the strata of age, BMI, hypertension, diabetes, TG/HDL-C, and alcohol intake. In particular, these associations were statistically stronger in men who smoked more than 20 cigarettes per day and had a BMI <23 kg/m2, hypertension, diabetes, or TG/HDL-C <3, or who did not drink alcohol.
- Bilirubin, which is a bile pigment, is generally regarded as a waste product of heme catabolism. However, it has been suggested that bilirubin might play an important role as an antioxidant, and its role as an antioxidant in vitro has recently been identified [24-28]. A number of recent in vitro studies have shown that bilirubin is more efficient than α-tocopherol at inhibiting low-density lipoprotein (LDL) oxidation and is a more efficient protector of human ventricular myocytes than either vitamin C or vitamin E [29-32]. Cigarette smoke contains a large quantity of free radicals, resulting in endothelial injury [33]. LDL oxidation appears as an early event of atherosclerosis and increases with cigarette smoking [34-36]. In this study, low serum bilirubin levels could have been caused by overconsumption of free-radicals produced mostly by cigarette smoking.
- This study has several limitations. Due to its cross-sectional design, the present study precluded the determination of causality. Bilirubin concentrations were measured only once. Another limitation may be that this study was performed only among men due to the small number of female Korean smokers. However, the main strength of this study is that to our knowledge it is a large sample size used to evaluate the inverse association between bilirubin concentration and cigarette smoking among Korean men. Most published studies have been limited to Caucasians rather than Asians. Second, Gilbert's syndrome is a genetic disorder of bilirubin metabolism that can result in production of elevated levels of indirect bilirubin in the bloodstream without any serious consequences [37]. In Korea, participants with Gilbert's syndrome have been shown to have a low prevalence and incidence of coronary heart diseases and higher levels of high density lipoprotein and antioxidant levels [38]. In this study, to clarify the results, only apparently healthy Korean men without a high possibility of having Gilbert's syndrome (total bilirubin concentrations >34.2 µol/L) [9] or any other diseases, which might affect the association between serum bilirubin and smoking, were included in the study. Still, total bilirubin concentrations >34.2 µol/L is not the definition or exclusion of Gilbert's syndrome. We also could not find any differences in the risk of having hypobilirubinemia when we included the participants with Gilbert's syndrome. The association between serum bilirubin and smoking remained significant after the exclusions. Finally, participants in the KMI study were mostly workers; therefore, they were mostly younger than those in the Korean National Health and Nutrition Examination Survey data.
- In conclusion, cigarette smoking decreases all three types of serum bilirubin in apparently health Korean men independently of hemoglobin. Bilirubin is inexpensive and easily measured in most clinical laboratories. Further studies are needed to determine if measuring bilirubin is effective in detecting free-radicals produced by smoking, which contribute to serious diseases including CVD. Additionally, further investigations should be carried out to determine whether such associations also exist among apparently healthy Korean women.
DISCUSSION
ACKNOWLEDGEMENTS
-
The authors have no conflicts of interest with the material presented in this paper.
-
This article is available at http://jpmph.org/.
Notes
- 1. Erhardt L. Cigarette smoking: an undertreated risk factor for cardiovascular disease. Atherosclerosis 2009;205(1):23-32. 19217623ArticlePubMed
- 2. World Health Organization. Tobacco control. 1999. Geneva: World Health Organization
- 3. Korean Ministry of Health and Welfare. The Korea National Health and Nutrition Examination Survey. 2007. Seoul: Korean Ministry of Health and Welfare
- 4. Stocker R, Glazer AN, Ames BN. Antioxidant activity of albumin-bound bilirubin. Proc Natl Acad Sci U S A 1987;84(16):5918-5922. 3475708ArticlePubMedPMC
- 5. Stocker R, Yamamoto Y, McDonagh AF, Glazer AN, Ames BN. Bilirubin is an antioxidant of possible physiological importance. Science 1987;235(4792):1043-1046. 3029864ArticlePubMed
- 6. Wu TW, Wu J, Li RK, Mickle D, Carey D. Albumin-bound bilirubins protect human ventricular myocytes against oxyradical damage. Biochem Cell Biol 1991;69(10-11):683-688. 1799433ArticlePubMed
- 7. Schwertner HA, Vitek L. Gilbert syndrome, UGT1A1*28 allele, and cardiovascular disease risk: possible protective effects and therapeutic applications of bilirubin. Atherosclerosis 2008;198(1):1-11. 18343383ArticlePubMed
- 8. Kimm H, Yun JE, Jo J, Jee SH. Low serum bilirubin level as an independent predictor of stroke incidence: a prospective study in Korean men and women. Stroke 2009;40(11):3422-3427. 19713538ArticlePubMed
- 9. Lin LY, Kuo HK, Hwang JJ, Lai LP, Chiang FT, Tseng CD, et al. Serum bilirubin is inversely associated with insulin resistance and metabolic syndrome among children and adolescents. Atherosclerosis 2009;203(2):563-568. 18775539ArticlePubMed
- 10. Jo J, Yun JE, Lee H, Kimm H, Jee SH. Total, direct, and indirect serum bilirubin concentrations and metabolic syndrome among the Korean population. Endocrine 2011;39(2):182-189. 21116740ArticlePubMed
- 11. Chan-Yeung M, Ferreira P, Frohlich J, Schulzer M, Tan F. The effects of age, smoking, and alcohol on routine laboratory tests. Am J Clin Pathol 1981;75(3):320-326. 7211753PubMed
- 12. Hopkins PN, Wu LL, Hunt SC, James BC, Vincent GM, Williams RR. Higher serum bilirubin is associated with decreased risk for early familial coronary artery disease. Arterioscler Thromb Vasc Biol 1996;16(2):250-255. 8620339ArticlePubMed
- 13. Schwertner HA. Association of smoking and low serum bilirubin antioxidant concentrations. Atherosclerosis 1998;136(2):383-387. 9543110ArticlePubMed
- 14. Van Hoydonck PG, Temme EH, Schouten EG. Serum bilirubin concentration in a Belgian population: the association with smoking status and type of cigarettes. Int J Epidemiol 2001;30(6):1465-1472. 11821365ArticlePubMed
- 15. Micozzi MS, Albanes D, Stevens RG. Relation of body size and composition to clinical biochemical and hematologic indices in US men and women. Am J Clin Nutr 1989;50(6):1276-1281. 2596419PubMed
- 16. Milman N, Byg KE, Mulvad G, Pedersen HS, Bjerregaard P. Haemoglobin concentrations appear to be lower in indigenous Greenlanders than in Danes: assessment of haemoglobin in 234 Greenlanders and in 2804 Danes. Eur J Haematol 2001;67(1):23-29. 11553263ArticlePubMed
- 17. Caliskan M, Erdogan D, Gullu H, Tok D, Bilgi M, Muderrisoglu H. Low serum bilirubin concentrations are associated with impaired aortic elastic properties, but not impaired left ventricular diastolic function. Int J Clin Pract 2007;61(2):218-224. 21882369ArticlePubMed
- 18. Pineda S, Bang OY, Saver JL, Starkman S, Yun SW, Liebeskind DS, et al. Association of serum bilirubin with ischemic stroke outcomes. J Stroke Cerebrovasc Dis 2008;17(3):147-152. 18436156ArticlePubMedPMC
- 19. Hwang HJ, Kim SH. Inverse relationship between fasting direct bilirubin and metabolic syndrome in Korean adults. Clin Chim Acta 2010;411(19-20):1496-1501. 20542021ArticlePubMed
- 20. Nakagami T, Toyomura K, Kinoshita T, Morisawa S. A beneficial role of bile pigments as an endogenous tissue protector: anti-complement effects of biliverdin and conjugated bilirubin. Biochim Biophys Acta 1993;1158(2):189-193. 8399320ArticlePubMed
- 21. Mamtani M, Patel A, Renge R, Kulkarni H. Prognostic value of direct bilirubin in neonatal hyperbilirubinemia. Indian J Pediatr 2007;74(9):819-822. 17901666ArticlePubMed
- 22. Shiomi S, Habu D, Kuroki T, Ishida S, Tatsumi N. Clinical usefulness of conjugated bilirubin levels in patients with acute liver diseases. J Gastroenterol 1999;34(1):88-93. 10204616ArticlePubMed
- 23. Li B, Wang Z, Fang JJ, Xu CY, Chen WX. Evaluation of prognostic markers in severe drug-induced liver disease. World J Gastroenterol 2007;13(4):628-632. 17278233ArticlePubMedPMC
- 24. Frei B, Stocker R, Ames BN. Antioxidant defenses and lipid peroxidation in human blood plasma. Proc Natl Acad Sci U S A 1988;85(24):9748-9752. 3200852ArticlePubMedPMC
- 25. Hidalgo FJ, Zamora R, Dillard CJ, Tappel AL. Can serum bilirubin be an index of in vivo oxidative stress? Med Hypotheses 1990;33(3):207-211. 2292986ArticlePubMed
- 26. Yamaguchi T, Horio F, Hashizume T, Tanaka M, Ikeda S, Kakinuma A, et al. Bilirubin is oxidized in rats treated with endotoxin and acts as a physiological antioxidant synergistically with ascorbic acid in vivo. Biochem Biophys Res Commun 1995;214(1):11-19. 7669030ArticlePubMed
- 27. Yamaguchi T, Hashizume T, Tanaka M, Nakayama M, Sugimoto A, Ikeda S, et al. Bilirubin oxidation provoked by endotoxin treatment is suppressed by feeding ascorbic acid in a rat mutant unable to synthesize ascorbic acid. Eur J Biochem 1997;245(2):233-240. 9151948ArticlePubMed
- 28. Minetti M, Mallozzi C, Di Stasi AM, Pietraforte D. Bilirubin is an effective antioxidant of peroxynitrite-mediated protein oxidation in human blood plasma. Arch Biochem Biophys 1998;352(2):165-174. 9587403ArticlePubMed
- 29. Wu TW, Fung KP, Yang CC. Unconjugated bilirubin inhibits the oxidation of human low density lipoprotein better than Trolox. Life Sci 1994;54(25):P477-P481. 8201841ArticlePubMed
- 30. Wu TW, Fung KP, Wu J, Yang CC, Weisel RD. Antioxidation of human low density lipoprotein by unconjugated and conjugated bilirubins. Biochem Pharmacol 1996;51(6):859-862. 8602883ArticlePubMed
- 31. Neuzil J, Stocker R. Free and albumin-bound bilirubin are efficient co-antioxidants for alpha-tocopherol, inhibiting plasma and low density lipoprotein lipid peroxidation. J Biol Chem 1994;269(24):16712-16719. 8206992PubMed
- 32. Hulea SA, Wasowicz E, Kummerow FA. Inhibition of metal-catalyzed oxidation of low-density lipoprotein by free and albumin-bound bilirubin. Biochim Biophys Acta 1995;1259(1):29-38. 7492612ArticlePubMed
- 33. Sull JW, Kim HJ, Yun JE, Park EJ, Kim G, Jee SH. Serum adiponectin is associated with smoking status in healthy Korean men. Endocr J 2009;56(1):73-78. 18840926ArticlePubMed
- 34. Frei B, Forte TM, Ames BN, Cross CE. Gas phase oxidants of cigarette smoke induce lipid peroxidation and changes in lipoprotein properties in human blood plasma. Protective effects of ascorbic acid. Biochem J 1991;277(Pt 1):133-138. 1854329PubMedPMC
- 35. Frei B. Reactive oxygen species and antioxidant vitamins: mechanisms of action. Am J Med 1994;97(3A):5S-13S. 8085584Article
- 36. Scheffler E, Wiest E, Woehrle J, Otto I, Schulz I, Huber L, et al. Smoking influences the atherogenic potential of low-density lipoprotein. Clin Investig 1992;70(3-4):263-268ArticlePubMed
- 37. Burchell B, Hume R. Molecular genetic basis of Gilbert's syndrome. J Gastroenterol Hepatol 1999;14(10):960-966. 10530490ArticlePubMed
- 38. Yoon SJ, Lee HS, Lee SW, Yun JE, Kim SY, Cho ER, et al. The association between adiponectin and diabetes in the Korean population. Metabolism 2008;57(6):853-857. 18502270ArticlePubMed
REFERENCES
| Cigarette smoking |
Serum bilirubin subtypes |
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n |
Total bilirubin |
Direct bilirubin |
Indirect bilirubin |
|||||||
| n1 | Model I2 | Model II3 | n1 | Model I2 | Model II3 | n1 | Model I2 | Model II3 | ||
| Smoking amount (cigarette/d) | ||||||||||
| Never smoker | 14 992 | 2896 | 1.0 | 1.0 | 3397 | 1.0 | 1.0 | 1927 | 1.0 | 1.0 |
| 1 - 9 | 4535 | 916 | 1.1 (1.0, 1.2) | 1.2 (1.1, 1.3) | 1056 | 1.2 (1.1, 1.3) | 1.2 (1.1, 1.3) | 612 | 1.1 (1.0, 1.2) | 1.1 (1.0, 1.2) |
| 10 - 19 | 15 481 | 3799 | 1.5 (1.4, 1.6) | 1.6 (1.5, 1.7) | 4080 | 1.4 (1.3, 1.5) | 1.5 (1.4, 1.5) | 2679 | 1.5 (1.4, 1.6) | 1.6 (1.5, 1.7) |
| ≥20 | 10 151 | 2765 | 1.8 (1.6, 1.9) | 1.9 (1.8, 2.0) | 2966 | 1.7 (1.6, 1.8) | 1.8 (1.7, 1.9) | 1950 | 1.7 (1.6, 1.8) | 1.9 (1.7, 2.0) |
| Smoking duration (y) | ||||||||||
| Never smoker | 14 992 | 2896 | 1.0 | 1.0 | 3397 | 1.0 | 1.0 | 1927 | 1.0 | 1.0 |
| 1 - 12 | 8047 | 1631 | 1.1 (1.1, 1.2) | 1.1 (1.1, 1.2) | 1814 | 1.1 (1.1, 1.2) | 1.1 (1.1, 1.2) | 1106 | 1.1 (1.0, 1.2) | 1.1 (1.0, 1.2) |
| 13 - 21 | 16 501 | 4022 | 1.5 (1.4, 1.6) | 1.5 (1.4, 1.6) | 4301 | 1.4 (1.3, 1.5) | 1.4 (1.3, 1.5) | 2835 | 1.5 (1.4, 1.6) | 1.5 (1.4, 1.6) |
| ≥22 | 8254 | 2279 | 1.9 (1.8, 2.0) | 1.9 (1.8, 2.0) | 2458 | 1.8 (1.7, 1.9) | 1.8 (1.7, 1.9) | 1608 | 1.8 (1.7, 2.0) | 1.8 (1.7, 2.0) |
| Pack-years4 | ||||||||||
| Never smoker | 14 992 | 2896 | 1.0 | 1.0 | 3397 | 1.0 | 1.0 | 1927 | 1.0 | 1.0 |
| 1 - 6 | 7360 | 1511 | 1.1 (1.1, 1.2) | 1.2 (1.1, 1.3) | 1695 | 1.1 (1.0, 1.2) | 1.2 (1.1, 1.3) | 1011 | 1.1 (1.0, 1.2) | 1.1 (1.0, 1.2) |
| 7 - 19 | 14 548 | 3585 | 1.4 (1.4, 1.5) | 1.6 (1.5, 1.6) | 3827 | 1.4 (1.3, 1.4) | 1.5 (1.4, 1.5) | 2552 | 1.4 (1.3, 1.5) | 1.6 (1.5, 1.7) |
| ≥20 | 7576 | 2200 | 1.7 (1.6, 1.9) | 2.1 (1.9, 2.2) | 2376 | 1.5 (1.4, 1.6) | 1.9 (1.8, 2.0) | 1548 | 1.7 (1.6, 1.9) | 2.0 (1.9, 2.2) |
1 The number of the lowest quartile of bilirubin subtypes (total bilirubin, direct bilirubin, indirect bilirubin).
2 Adjusted for age, alanine aminotransferase, gamma-glutamyltransferase, uric acid, body mass index, and alcohol consumption.
3 Adjusted for age, alanine aminotransferase, gamma-glutamyltransferase, uric acid, body mass index, alcohol consumption and hemoglobin.
4 Pack-years were calculated as amount (cigarettes/d) x period of smoking (y)/20.
| Variables |
Smoking amount (cigarette/d) |
||||||
|---|---|---|---|---|---|---|---|
| NS1 |
1-9 |
10 - 19 |
≥ 20 |
||||
| n | OR (95% CI) | n | OR (95% CI) | n | OR (95% CI) | ||
| Age (y) | |||||||
| < 40 | 7305 | 2597 | 1.1 (0.9, 1.2) | 8134 | 1.4 (1.3, 1.5) | 3548 | 1.6 (1.4, 1.7) |
| ≥40 | 7687 | 1938 | 1.1 (1.0, 1.3) | 7347 | 1.4 (1.3, 1.5) | 6603 | 1.6 (1.5, 1.7) |
| BMI (kg/m2) | |||||||
| < 23 | 10 221 | 1592 | 1.1 (0.9, 1.2) | 4975 | 1.5 (1.4, 1.7) | 2782 | 1.8 (1.7, 2.1) |
| ≥23 | 22 827 | 2943 | 1.1 (1.0, 1.2) | 10 506 | 1.3 (1.2, 1.4) | 7369 | 1.5 (1.4, 1.6) |
| Hypertension | |||||||
| No | 12 869 | 3985 | 1.2 (0.9, 1.5) | 13 464 | 1.2 (1.1, 1.4) | 8484 | 1.4 (1.2, 1.6) |
| Yes | 2123 | 550 | 1.1 (1.0, 1.2) | 2017 | 1.4 (1.3, 1.5) | 1667 | 1.6 (1.5, 1.7) |
| Diabetes | |||||||
| No | 14 445 | 4403 | 1.3 (0.8, 1.9) | 14 911 | 1.2 (1.0, 1.6) | 9506 | 1.5 (1.2, 1.9) |
| Yes | 547 | 132 | 1.1 (1.0, 1.2) | 570 | 1.4 (1.3, 1.5) | 645 | 1.6 (1.5, 1.7) |
| TG/HDL-C (mg/dL) | |||||||
| <3 | 8990 | 2551 | 1.2 (1.1, 1.3) | 7721 | 1.4 (1.3, 1.5) | 4474 | 1.6 (1.5, 1.7) |
| ≥3 | 6002 | 1984 | 1.0 (0.9, 1.1) | 7760 | 1.3 (1.2, 1.4) | 5677 | 1.5 (1.4, 1.6) |
| Alcohol intake | |||||||
| No | 3106 | 379 | 1.0 (0.8, 1.3) | 1279 | 1.9 (1.6, 2.1) | 1055 | 1.9 (1.7, 2.2) |
| Yes | 11 731 | 4110 | 1.1 (1.0, 1.2) | 14 045 | 1.4 (1.3, 1.5) | 8942 | 1.6 (1.5, 1.7) |
Figure & Data
References
Citations
- Association between elevated serum bilirubin levels with preserved lung function under conditions of exposure to air pollution
Udi Shapira, Rafael Y. Brezinski, Ori Rogowski, David Zeltser, Shlomo Berliner, Itzhak Shapira, Shani Shenhar-Tsarfaty, Elizabeth Fireman
BMC Pulmonary Medicine.2021;[Epub] CrossRef - ROLE OF BILIRUBIN AS A POTENTIALANTIOXIDANT IN SMOKERS
Varshini. S, A. Preethi, G. Udayakumari
INTERNATIONAL JOURNAL OF SCIENTIFIC RESEARCH.2021; : 43. CrossRef - Direct Bilirubin Levels and Risk of Metabolic Syndrome in Healthy Chinese Men
Xiao-Hong Li, Hai-Yan Lin, Li-Ying Guan, Hui Peng, Meng-Meng Wen, Yong-Qian Cao, Xiu-Yun Jiang, Yi-Bing Wang
BioMed Research International.2017; 2017: 1. CrossRef - Serum bilirubin levels are inversely associated with PAI-1 and fibrinogen in Korean subjects
Hyun Sun Cho, Sung Won Lee, Eun Sook Kim, Juyoung Shin, Sung Dae Moon, Je Ho Han, Bong Yun Cha
Atherosclerosis.2016; 244: 204. CrossRef - Active and Passive Smoking and Serum Total Bilirubin in a Rural Korean Population
Na Hyun Kim, Hyeon Chang Kim, Joo Young Lee, Ju-Mi Lee, Il Suh
Nicotine & Tobacco Research.2016; 18(5): 572. CrossRef - Cigarette smoking behaviour and blood metabolomics
Fangyi Gu, Andriy Derkach, Neal D Freedman, Maria Teresa Landi, Demetrius Albanes, Stephanie J Weinstein, Alison M Mondul, Charles E Matthews, Kristin A Guertin, Qian Xiao, Wei Zheng, Xiao-ou Shu, Joshua N Sampson, Steven C Moore, Neil E Caporaso
International Journal of Epidemiology.2016; 45(5): 1421. CrossRef - Cigarette Smoking Habit and Subjective Quality of Sleep
Alimohamad Asghari, Seyed Kamran Kamrava, Mohsen Rezaee Hemami, Maryam Jalessi, Parin Yazdanifard, Mohammad Farhadi, Seyed Behzad Pousti, Seyed Saleh Tabatabaie
Scimetr.2015;[Epub] CrossRef - Serum Bilirubin Levels Predict Future Development of Metabolic Syndrome in Healthy Middle-aged Nonsmoking Men
Shao-Sung Huang, Wan-Leong Chan, Hsin-Bang Leu, Po-Hsun Huang, Shing-Jong Lin, Jaw-Wen Chen
The American Journal of Medicine.2015; 128(10): 1138.e35. CrossRef - Serum bilirubin concentration is modified by UGT1A1 Haplotypes and influences risk of Type-2 diabetes in the Norfolk Island genetic isolate
M. C. Benton, R. A. Lea, D. Macartney-Coxson, C. Bellis, M. A. Carless, J. E. Curran, M. Hanna, D. Eccles, G. K. Chambers, J. Blangero, L. R. Griffiths
BMC Genetics.2015;[Epub] CrossRef - Serum Bilirubin and Disease Progression in Mild COPD
Scott Apperley, Hye Yun Park, Daniel T. Holmes, S. F. Paul Man, Donald Tashkin, Robert A. Wise, John E. Connett, Don D. Sin
Chest.2015; 148(1): 169. CrossRef - Smoking Cessation Is Followed by Increases in Serum Bilirubin, an Endogenous Antioxidant Associated With Lower Risk of Lung Cancer and Cardiovascular Disease
Stephanie S. O’Malley, Ran Wu, Susan T. Mayne, Peter I. Jatlow
Nicotine & Tobacco Research.2014; 16(8): 1145. CrossRef - Combined Effects of Smoking and Bilirubin Levels on the Risk of Lung Cancer in Korea: The Severance Cohort Study
Jung-eun Lim, Heejin Kimm, Sun Ha Jee, Suminori Akiba
PLoS ONE.2014; 9(8): e103972. CrossRef - The Relationship between Total Bilirubin Levels and Total Mortality in Older Adults: The United States National Health and Nutrition Examination Survey (NHANES) 1999-2004
Kwok-Leung Ong, Matthew A. Allison, Bernard M. Y. Cheung, Ben J. Wu, Philip J. Barter, Kerry-Anne Rye, Shree Ram Singh
PLoS ONE.2014; 9(4): e94479. CrossRef - The Association Between Heterozygosity forUGT1A1*6,UGT1A1*28, and Variation in the Serum Total-Bilirubin Level in Healthy Young Japanese Adults
Hiroyuki Moriya, Katsuhiko Saito, Nuala Helsby, Shigekazu Sugino, Michiaki Yamakage, Masahiko Takasaki, Hidenori Kato, Nahoko Kurosawa
Genetic Testing and Molecular Biomarkers.2013; 17(6): 464. CrossRef - Serum bilirubin may serve as a marker for increased heme oxygenase activity and inducibility in tissues – A rationale for the versatile health protection associated with elevated plasma bilirubin
Mark F. McCarty
Medical Hypotheses.2013; 81(4): 607. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite