Articles
- Page Path
- HOME > J Prev Med Public Health > Volume 57(3); 2024 > Article
-
Original Article
Prevalence and Factors Associated With Adolescent Pregnancy Among an Indigenous Ethnic Group in Rural Nepal: A Community-based Cross-sectional Study -
Kusumsheela Bhatta
 , Pratiksha Pathak, Madhusudan Subedi
, Pratiksha Pathak, Madhusudan Subedi -
Journal of Preventive Medicine and Public Health 2024;57(3):269-278.
DOI: https://doi.org/10.3961/jpmph.24.023
Published online: April 26, 2024
School of Public Health, Patan Academy of Health Sciences, Lalitpur, Nepal
- Corresponding author: Kusumsheela Bhatta, School of Public Health, Patan Academy of Health Sciences, Lagankhel, Lalitpur 44700, Nepal E-mail: mph.kusumsheelabhatta@pahs.edu.np
Copyright © 2024 The Korean Society for Preventive Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Objectives:
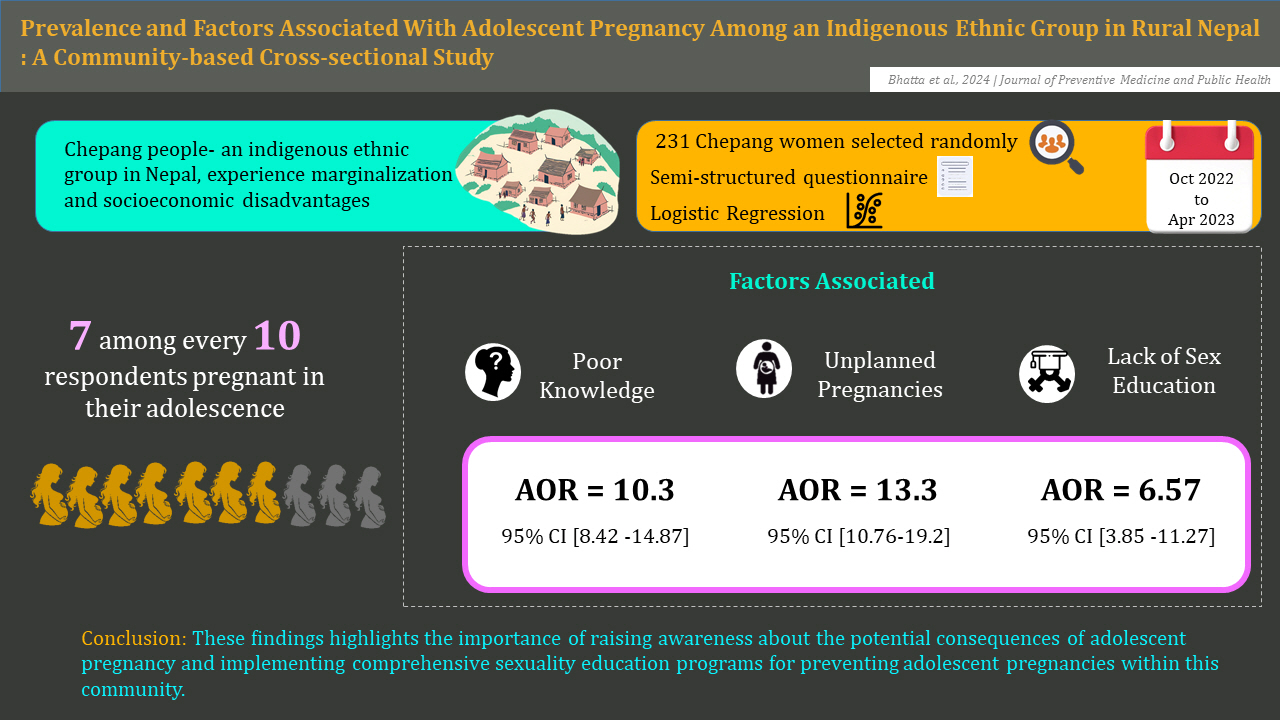
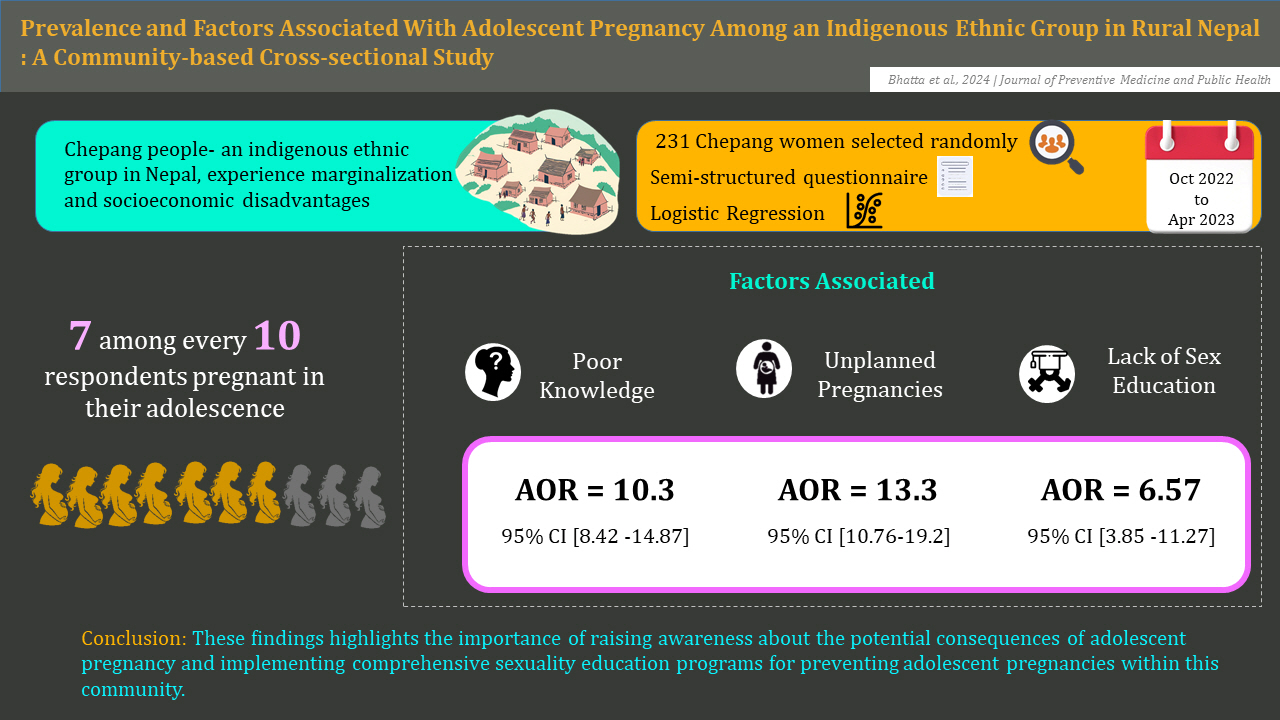
- The Chepang people, an indigenous ethnic group in Nepal, experience substantial marginalization and socioeconomic disadvantages, making their communities among the most vulnerable in the region. This study aimed to determine the prevalence and factors associated with adolescent pregnancy in the Chepang communities of Raksirang Rural Municipality, Makwanpur District, Bagmati Province, Nepal.
-
Methods:
- A cross-sectional study was conducted from October 2022 to April 2023 among 231 Chepang women selected using simple random sampling from Raksirang Rural Municipality. A semi-structured questionnaire was used for interviewing the mothers. Bivariate and multivariate logistic regression analyses were performed, using odds ratios with 95% confidence intervals (CIs). Variables with a variation inflation factor of more than 2 and a p-value of more than 0.25 were excluded from the final model.
-
Results:
- The study revealed that the prevalence rate of adolescent pregnancy among Chepang women was 71.4% (95% CI, 65.14 to 77.16). A large percentage of participants (72.7%) were married before the age of 18 years. Poor knowledge of adolescent pregnancy (adjusted odds ratio [aOR], 10.3; 95% CI, 8.42 to 14.87), unplanned pregnancy (aOR, 13.3; 95% CI, 10.76 to 19.2), and lack of sex education (aOR, 6.57; 95% CI, 3.85 to 11.27) were significantly associated with adolescent pregnancy.
-
Conclusions:
- The prevalence of adolescent pregnancy among the Chepang community was high. These findings highlighted the importance of raising awareness about the potential consequences of adolescent pregnancy and implementing comprehensive sexuality education programs for preventing adolescent pregnancies within this community.
- Keywords: Adolescent, Pregnancy, Prevalence, Ethnicity, Nepal
- Adolescent pregnancy, which is defined as any pregnancy in girls and women aged 10-19 years, is a matter of concern for public health and human rights. In developing countries, 20 000 girls younger than 18 years old give birth each day, and 95% of the world’s births to adolescents take place in low and middle-income countries [1]. The adolescent fertility rate in South Asia is 26 births per 1000 girls aged 15-19 years, which is ranked second globally after the sub-Saharan Africa region [2]. In Nepal, after declining between 2001 (21%) and 2011 (17%), the rate of teenage childbirth remained constant from 2011 to 2016 (17%). The rate has declined subsequently to 14% as per the Nepal Demographic and Health Survey (NDHS) 2022 [3,4].
- Maternal conditions are the leading causes of disability and death in women aged 15-19 years, with adolescent mothers at higher risk for complications such as eclampsia, endometritis, infections, tears, obstructed labor, and premature membrane rupture [5,6].
- Factors associated with adolescent pregnancy include low socioeconomic status (SES), unemployment, a low educational level, a lack of access to media exposure regarding public health issues, unplanned pregnancy, early marriage, sexual risk behaviors, family experience of adolescent birth, peer pressure, and a lack of sex education and healthcare service [7-9]. In Nepal, marrying at an early age is linked with a higher likelihood of adolescent pregnancy, with more than one-third of women who marry before their 15th birthday having 3 or more children. In contrast, only 1% of women who married as adults have as many children [10].
- The Chepang people are one of the highly marginalized groups living on the hilly and steeper slopes primarily in the Chitwan, Dhading, Gorkha, and Makawanpur Districts of Nepal [11]. Chepang communities in Nepal, comprising 84 364 individuals, constitute approximately 0.29% of the total national population [12]. The Chepang population in Raksirang Rural Municipality is 11 427 individuals, of whom 5792 are men and 5635 are women [13]. The Chepang people, who refer to themselves as Chyobang, derive their name from “chyo,” meaning “on the top,” and “bang,” meaning “stone,” indicating a belief that their ancestors resided in rock shelters and caves, often attributing their origin to stone [14]. The socioeconomic structure of the Chepang people is divided into two groups: the Kachhare, who have no sub-clans and are considered “pure” Chepang, and the Pukunthali, who are organized into subclans that have supposedly “mixed” with neighboring populations [15]. The Chepangs share ancestral ties with Tibetans and are characterized by short and flat noses, round faces, dark and brown complexion, thin to medium ears, dark eyes, prominent eyebrows, and medium height [16]. In the past few generations, the Chepangs, also known as “prajas” (political subjects), have gradually moved away from their semi-nomadic, slash-and-burn lifestyle to a more settled one, relying more on permanent fields for maize, millet, and bananas, rather than solely depending on natural forest resources as before [17].
- No prior studies have accounted for the factors associated with adolescent pregnancy in Chepang communities, where early marriage and pregnancy are still preferred by cultural norms. In this context, our community-based study aimed to determine the prevalence and factors associated with adolescent pregnancy among Chepang women of the Raksirang Rural Municipality, Makwanpur District, Nepal, to provide evidence and support for improving future efforts to reduce its prevalence.
INTRODUCTION
- Study Design
- A 6-month cross-sectional study was undertaken from October 2022 to April 2023 to determine the prevalence and factors associated with adolescent pregnancy among Chepang women in Raksirang Rural Municipality, Makwanpur District, Bagmati Province. The study was conducted in Wards 5 and 8 of Raksirang Rural Municipality due to both the region’s reportedly high density of Chepang residents and the feasibility of research, considering the extreme geographical terrain.
- Study Population
- Information was collected from Chepang women of Wards 5 and 8 in Raksirang Rural Municipality aged 10 years to 25 years who had given birth at least once before the preparation of the sampling frame. Individuals who did not give consent to participate in the study, were seriously ill, or had communication difficulties due to speaking and hearing impairment were excluded from the study. The study adopted a retrospective approach to data collection in considering the inclusion of participants. Within this group, pregnancies that had occurred when the mother was between 10 years and 19 years of age were classified as adolescent pregnancies.
- The required sample size was calculated to be 231 individuals using the single population proportion formula, with the following statistical assumptions: a 5% margin of error (0.05), a Z-value of 1.96 corresponding to a 95% confidence interval (CI), a design effect of 1.5, a non-response rate of 10.0%, and a proportion of 10.1% of the women in Bagmati Province, Nepal who were aged 15-19 years and had begun bearing children according to the NDHS 2016 [4].
- After obtaining ethical approval from the Institutional Review Committee (IRC), the researchers communicated with female community health volunteers and residents of Wards 5 and 8 and requested that they provide the names, ages, and localities of individuals who met the study’s inclusion criteria. Thus, a list of 276 Chepang mothers aged 10 years to 25 years who met the study’s inclusion criteria was prepared. The Microsoft Excel RANDBETWEEN function was used to select the 231 participants randomly.
- Variables
- The independent variables of the study were the participant’s educational level, their husband’s educational level, family size, occupation, SES, use of contraceptives, unplanned pregnancy, knowledge regarding adolescent pregnancy, marriage type, family influence, peer influence, awareness of sex education, access to contraceptives, distance to the nearest healthcare facility, and decision-making power.
- The dependent variable of the study was adolescent pregnancy, which was defined as any pregnancy from a girl or woman who was aged 10-19 years at the time the baby was born [18].
- SES was assessed using Kuppuswamy’s SES scale, modified within the context of Nepal. The scale measures SES based on the education and occupation of the household head and the monthly family income. The results were divided initially into 5 socioeconomic classes: upper (I) (score: 26-29), upper middle (II) (score: 16-25), lower middle (III) (score:11-15), upper lower (IV) (score: 5-10), and lower (V) (score: <5) [19]. The knowledge questionnaire about early pregnancy had 9 questions with “right,” “wrong,” and “I do not know” answers, adapted from a cross-sectional study conducted in healthcare centers in Tabriz, Iran. The content validity ratio and content validity index of the tool were 0.88 and 0.84, respectively. The knowledge score was categorized into 3 levels for analysis: good (score: 7-9), average (score: 4-6), and poor (score: 0-3) [20].
- Data Collection Tools
- A semi-structured questionnaire divided into 5 parts was used for interviewing the participants. The first part of the tool contained socio-demographic variables. The second part included pregnancy and marriage-related information, such as the participant’s age at first marriage, marriage type, whether they wanted to be married, age at first pregnancy, and whether the pregnancy was planned. The third part of the tool assessed contraception-related information, including their knowledge, use, and decision-making regarding contraceptives. The fourth part of the tool assessed the participants’ knowledge of adolescent pregnancy. The fifth part included access-related information.
- Questions on socio-demographic factors were compiled from the 2016 NDHS, the World Health Organization’s STEPS survey 2019, and other adolescent pregnancy-related factors that were identified in the literature. A pilot test was conducted among 30 adolescent mothers, selected deliberately from Konjyosom Rural Municipality, Lalitpur District, Bagmati Province. Further, to ensure the face validity of the tool, participants were asked during pre-testing whether the construct measured what it intended to measure. Questions were forward-translated into the Nepali language and then backtranslated to English. Back-translated versions of the questions were compared with the original questions and finalized after discussion with the supervisors.
- Statistical Analysis
- The data were coded, entered in EpiData version 3.1 (EpiData Association, Odense, Denmark), and cleaned in Excel 2016 (Microsoft Corp., Redmond, WA, USA). The cleaned data were exported from Excel and analyzed using Stata/MP version 13 (StataCorp, College Station, TX, USA) and EZR 4.0.4 (Saitama Medical Center, Jichi Medical University, Saitama, Japan). Descriptive statistics were presented using frequency, percentage, mean and standard deviation, median, and interquartile range depending on the distribution of variables. The prevalence of adolescent pregnancy among Chepang women is presented in Table 1.
- A bivariate analysis of the independent variables was carried out with the dependent variable. For the variables found to be significant, multivariate logistic regression was performed to identify the independent predictor of the outcome variable. We adopted a rigorous variable selection process at each stage of our analysis, which incorporated 4 models of logistic regression. In the first model (fitted model 1), the sociodemographic variables were assessed. Fitted models 2 and 3 included the pregnancy and marriage-related variables and the contraception and access-related variables. In the fourth and final model, the socio-demographic, pregnancy and marriage-related, and contraception and access-related variables were simultaneously assessed in relation to the dependent variable.
- The p-values presented in Tables 2-4 show the results of the multivariate logistic regression analysis. The tables include both adjusted and unadjusted p-values, with the adjusted p-values representing the significance of each variable from the multivariate logistic regression analysis, and the unadjusted p-values reflecting their significance from the bivariate analysis.
- Multi-collinearity between variables was assessed through the variance inflation factor (VIF). Variables with a VIF of more than 2 and a p-value of more than 0.25 were excluded from the final model. The final model identified the factors associated with adolescent pregnancy among Chepang women.
- Ethics Statement
- The study was approved by the IRC of the Patan Academy of Health Sciences (IRC-PAHS reference: PHP2209061673.A1). Approval was also obtained from the Raksirang Municipality Office before the study began. For minor participants (less than 18 years old), the study’s purpose was explained in detail to each participant’s guardians. Informed written consent was obtained from the guardians before the research interview, and assent was obtained subsequently from each minor individual. Informed consent was obtained from eligible individuals aged 18 years or older.
METHODS
- Regarding the age at first pregnancy, which was also a dependent variable for this study, approximately 7 out of 10 participants (71.4%; 95% CI, 65.1 to 77.2) had been pregnant during their adolescence (aged 10-19 years). The median age at first pregnancy was 18 years old (Table 1).
- Table 2 shows the general characteristics of the participants who participated in the study. The median age was observed to be 21 years. Most participants had a basic educational level (73.2%), followed by secondary education (14.7%) and no education (12.1%). Two-thirds (66.7%) of the participants’ husbands had a basic educational level, followed by secondary education (20.7%) and no education (12.6%). Regarding their employment, most participants were in a single category that included semi-professional workers, clerical workers, shop owners, and farmers (95.2%). In addition, the majority of the participants’ SES scores were in the upper lower category (74.5%), followed by the lower middle (23.4%), upper middle (1.3%), and lower categories (0.9%). Thus, for further analysis, the upper middle and lower middle categories were merged as a new upper category, and the upper lower and lower categories were merged as a new lower category.
- In fitted model 1 for assessing multicollinearity, the VIF was less than 2, and the model fit the data (p<0.05) when the null and fitted models were compared. The area under the curve (AUC) of the model was 0.69 (95% CI, 0.61 to 0.77), and the accuracy of the model was 75.32%. After multivariate logistic regression, the husband’s level of education and the family size showed a significant association with adolescent pregnancy (Table 2).
- A large percentage of participants (72.7%) were married before the age of 18 years. The median age at time of marriage was 17 years. In contrast, just under a third (29.0%) of the participants’ husbands were married before the age of 18 years. Around 60% of the participants had had an unplanned pregnancy. Regarding any sort of influence or pressure to give birth, around one-third (32.0%) of the participants were influenced by their family to give birth, and around one-fourth (24.7%) of the participants were influenced by their peers to give birth (Table 3).
- In fitted model 2, the VIF remained below 2, indicating acceptable levels of multicollinearity. The model fit the data (p<0.05) when the null and fitted models were compared. The AUC of the model was 0.98 (95% CI, 0.96 to 0.99), and the accuracy of the model was 92.64%. After multivariate logistic regression, age at marriage, unplanned pregnancy, and knowledge regarding adolescent pregnancy were found to be significantly associated with the outcome variable (Table 3).
- Around two-fifths of the participants (39.4%) had poor knowledge regarding adolescent pregnancy, followed by average knowledge (31.2%) and good knowledge (29.4%). Likewise, most participants (95.7%) did not use any form of contraception after they were married and before they had given birth to their first child. Around two-thirds (66.7%) of the participants had to travel more than 30 minutes to reach the nearest healthcare institution, and slightly less than two-thirds of the participants (64.9%) had not received sex education (Table 4).
- In the third fitted model, the VIF was below 2, and the model fit the data (p<0.05) when the null and fitted models were compared. The AUC of the model was 0.78 (95% CI, 0.71 to 0.84), and the accuracy of the model was 76.62%. After the multivariate analysis, only the sex education variable was found to be significantly associated with adolescent pregnancy (Table 4).
- In the final stage of analysis, a multivariate logistic regression incorporating the variables from the first 3 fitted models was undertaken to identify the predictors of adolescent pregnancy. Variables with a p-value <0.25 from the fitted models were considered for inclusion. Multicollinearity was evaluated using the VIF, and variables exceeding a VIF of 2 and a p-value of 0.25 were excluded. Consequently, the family size, husband’s educational level, type of marriage, unplanned pregnancy, knowledge of adolescent pregnancy, contraceptive use, decision-making regarding contraceptive methods, and sex education were retained in the final model. The model fitted the data (p<0.05) when the null and fitted models were compared. The AUC of the final model was 0.98 (95% CI, 0.97 to 1.00), and the accuracy of the model was 95.24%. The final model revealed that unplanned pregnancy, knowledge regarding adolescent pregnancy, and sex education were independent predictors of adolescent pregnancy (Table 5).
- After we controlled for other variables, we found that participants who had unplanned pregnancies had 13.30 times higher odds (95% CI, 10.76 to 19.20; p<0.001) of having an adolescent pregnancy compared to those who had a planned pregnancy. Similarly, after controlling for other variables, those with poor knowledge scores had 10.30 times higher odds (95% CI, 8.42 to 14.87; p=0.008) of having an adolescent pregnancy, and those with average knowledge scores had 5.46 times higher odds (95% CI, 4.31 to 9.64; p<0.05), compared to those who had good knowledge scores. Furthermore, the participants who did not receive sex education had 6.57 times higher odds (95% CI, 3.85 to 11.27; p=0.008) of being pregnant in adolescence than those who received sex education (Table 5).
RESULTS
- Our study determined that the prevalence of adolescent pregnancy among Chepang women was 71.4% (95% CI, 65.1 to 77.2). This rate was almost 5 times higher than the national average (14%) reported in NDHS 2022, and 3 times higher than in Karnali Province (21%) [3]. It was also significantly higher than the rate reported by a meta-analysis of teenage pregnancy in Nepal, 2000-2020 (13.2%) [6]. The rate was also higher than the findings of studies conducted in other districts of Nepal [21,22]. At the global level, around 14% of teenage girls and young women worldwide reported having a baby before the age of 18 [23]. Compared with the rate of adolescent pregnancy among women aged 15-19 in India (7.9%), the rate in our study was significantly higher [24].
- Further investigation of the context-specific and ethnicity-specific studies from Nepal showed that the rate found by our study was closer to the findings from these studies. A descriptive research study among Chepang women in Korak Village Development Committee, Chitwan District showed that 58.1% of the participants had their first childbirth aged 17-19 years [8]. Another study conducted among 217 married women of Dalit groups showed that 42.9% of them had given birth to their first child during their teenage years, which suggested that the rate of adolescent pregnancy may be higher among specific ethnicities [9]. This is supported by the findings of a 12-month observational study in 12 hospitals in Nepal, which showed that women from disadvantaged ethnic groups have a higher likelihood of being adolescent mothers [25]. The findings from our study suggest that the prevalence of adolescent pregnancy is higher among Chepang women in Raksirang Rural Municipality than in other parts of Nepal or globally. This may be because Chepang is a highly marginalized and disadvantaged ethnic group in Nepal as compared to the national average. Meanwhile, it is important to consider the influence of methodological differences and variations in inclusion criteria from other studies.
- Additionally, unplanned pregnancy was identified as a factor associated with adolescent pregnancy in our study. This is in alignment with a study drawn from NDHS data, where more than two-fifths of the pregnant women reported experiencing an unintended pregnancy, and the likelihood of unintended pregnancy decreased as women’s age at first marriage increased [21]. Our finding is supported by global-level evidence, which indicated that among 21 million adolescent girls who have become pregnant in developing countries, 10 million of these pregnancies were unplanned [26]. The pilot study conducted for our research also indicated unplanned pregnancy as a significant predictor of adolescent pregnancy [27].
- In our study, a lack of sex education was found to be a significant predictor of adolescent pregnancy. This agrees with the finding from a systematic review investigating the determinants of adolescent pregnancy in sub-Saharan Africa, which identified a lack of comprehensive sex education as a major determinant [28]. Our findings are further supported by a comprehensive analysis of 64 studies, which described the positive outcomes of sex education programs implemented in schools [29]. They also align with a study that explored the impact of sex education on teenage pregnancy in secondary schools in Ghana and found that concealing education and knowledge about sex from young people made them more curious and vulnerable [30]. In addition, several studies have associated sex education with reduced teen birth rates [27,31,32]. In contrast, one study indicated that teenagers who were exposed to school-based sex education experienced slightly higher pregnancy rates than those who were not exposed, and another study concluded that sex education had no significant effect on adolescent pregnancy [33,34].
- Poor knowledge of adolescent pregnancy was another risk factor identified in our study, which was similar to the findings of a study from Sunsari District, Nepal [35]. In our study, around two-fifths of the participants (39.4%) had poor knowledge regarding adolescent pregnancy, followed by average knowledge (31.2%) and good knowledge (29.4%). A study conducted in Gorkha District, Nepal indicated that around 30% of the participants had inadequate knowledge of adolescent pregnancy [36], and in a study conducted in India, the proportion of poor knowledge was similar [37]. A study at selected government junior colleges in India found that 25% of the participants had inadequate knowledge of adolescent pregnancy, slightly lower than the percentage with poor knowledge in our study [38].
- The study has some limitations. The use of simple random sampling for selecting participants increased the representativeness of the sample and reduced the risk of selection bias. However, Wards 5 and 8 were chosen deliberately, which limits the generalizability of our findings beyond these wards. Since the study relies on self-reported data, issues may have occurred with recall bias, social desirability bias, and the underreporting of sensitive information. Moreover, the study included participants up to the age of 25 years, and most of them had had their first pregnancy while 14 years to 19 years old. Having to recall information from 5 years to 10 years earlier may have added recall bias to the data.
- Based on our findings, it is strongly recommended that appropriate measures be taken, such as empowering young people with knowledge of the consequences of early pregnancy and providing them with access to comprehensive and age-appropriate sex education. To reduce unplanned pregnancies, educating adolescents about the use of contraceptives and providing them with options for preventing unintended pregnancies should be a priority.
DISCUSSION
-
Conflict of Interest
The authors have no conflicts of interest associated with the material presented in this paper.
-
Funding
The study received funding from the Nepal Health Research Council.
-
Author Contributions
Conceptualization: Bhatta K, Subedi M, Pathak P. Data curation: Bhatta K. Formal analysis: Bhatta K, Subedi M. Funding acquisition: Bhatta K, Subedi M. Methodology: Bhatta K, Pathak P. Project administration: Bhatta K. Visualization: Pathak P, Subedi M. Writing – original draft: Bhatta K. Writing – review & editing: Bhatta K, Subedi M, Pathak P.
Notes
Acknowledgements
| Age at first pregnancy (y) | Frequency (n) | % (95% CI) |
|---|---|---|
| 10-19 | 165 | 71.4 (65.1, 77.2) |
| ≥20 | 66 | 28.6 (22.8, 34.9) |
- 1. United Nations Population Fund (UNFPA). Adolescent pregnancy [cited 2023 Feb 8]. Available from: https://www.unfpa.org/adolescent-pregnancy#readmore-expand
- 2. Loaiza E, Liang M. Adolescent pregnancy: a review of the evidence; 2013 [cited 2022 Sep 10]. Available from: https://www.unfpa.org/sites/default/files/pub-pdf/ADOLESCENT%20PREGNANCY_UNFPA.pdf
- 3. Ministry of Health and Population, New ERA, ICF. Nepal Demographic and Health Survey 2022: key indicators report [cited 2023 Jan 22]. Available from: https://dhsprogram.com/pubs/pdf/PR142/PR142.pdf
- 4. Ministry of Health, New ERA, ICF. Nepal Demographic and Health Survey 2016; 2017 [cited 2023 Apr 5]. Available from: https://www.dhsprogram.com/pubs/pdf/FR336/FR336.pdf
- 5. United Nations Children’s Fund (UNICEF). Early childbearing; 2021 [cited 2022 Jun 10]. Available from: https://data.unicef.org/topic/child-health/adolescent-health/
- 6. Shrestha DB, Budhathoki P, Shrestha O, Karki S, Thapa N, Dangal G, et al. Teenage pregnancy and associated risk factors and outcome in Nepal from 2000-2020: a systematic review and meta-analysis. Kathmandu Univ Med J 2022;20(2):225-233. https://doi.org/10.3126/kumj.v20i2.51406Article
- 7. Poudel S, Upadhaya N, Khatri RB, Ghimire PR. Trends and factors associated with pregnancies among adolescent women in Nepal: pooled analysis of Nepal Demographic and Health Surveys (2006, 2011 and 2016). PLoS One 2018;13(8):e0202107. https://doi.org/10.1371/journal.pone.0202107ArticlePubMedPMC
- 8. Chung HW, Kim EM, Lee JE. Comprehensive understanding of risk and protective factors related to adolescent pregnancy in low- and middle-income countries: a systematic review. J Adolesc 2018;69: 180-188. https://doi.org/10.1016/j.adolescence.2018.10.007ArticlePubMedPMC
- 9. Koirala S, Poudel EN, Koirala A, Shrestha N. Factors influencing teenage pregnancy among Dalit ethnic groups in Bharatpur Metropolitian city, Chitwan. J Chitwan Med Coll 2021;11(3):21-25. https://doi.org/10.54530/jcmc.485Article
- 10. United Nations Children’s Fund (UNICEF). Ending child marriage: progress and prospects; 2014 [cited 2022 Dec 18]. Available from: https://data.unicef.org/resources/ending-childmarriage-progress-and-prospects/
- 11. Sharma G, Aryal B. Household economies of Chepang people in Chitwan. Econ Lit 2016;13: 39-45. https://doi.org/10.3126/el.v13i0.19149Article
- 12. Government of Nepal. National population and housing census 2021 (national report). Kathmandu: National Statistics Office; 2022
- 13. National Statistics Office. National population and housing census 2021: caste/ethnicity report: 2022 [cited 2024 May 16]. Available from: https://censusnepal.cbs.gov.np/results/downloads/caste-ethnicity
- 14. Rai NK. People of the stones, the Chepangs of central Nepal. Kathmandu: Tribhuvan University; 1985. p. 120-125
- 15. Viel A. Preliminary note on the Chepang of Nepal and their territory. Geneva: Arts & Cultures; 2020. p. 228-239
- 16. Khanal B. Social exclusion of the Chepangs in the era of postpolitical revolution in Nepal - a case study of Dhading district [dissertation]. Bergen: University of Bergen; 2014
- 17. Ghimire MN. Health status of children of Chepang and other communities of Nepal. J Adv Acad Res 2014;1(1):24-28ArticlePDF
- 18. Ganchimeg T, Ota E, Morisaki N, Laopaiboon M, Lumbiganon P, Zhang J, et al. Pregnancy and childbirth outcomes among adolescent mothers: a World Health Organization multicountry study. BJOG 2014;121 Suppl 1: 40-48. https://doi.org/10.1111/1471-0528.12630ArticlePubMed
- 19. Joshi SK, Acharya K. Modification of Kuppuswamy’s socioeconomic status scale in the context of Nepal, 2019. Kathmandu Univ Med J 2019;17(65):1-2
- 20. Naghizadeh S, Mirghafourvand M. Knowledge and attitudes of adolescent girls and their mothers about early pregnancy: a cross-sectional study. BMC Pregnancy Childbirth 2022;22(1):205. https://doi.org/10.1186/s12884-022-04551-zArticlePubMedPMC
- 21. Adhikari R, Soonthorndhada K, Prasartkul P. Correlates of unintended pregnancy among currently pregnant married women in Nepal. BMC Int Health Hum Rights 2009;9: 17. https://doi.org/10.1186/1472-698X-9-17ArticlePubMedPMC
- 22. Lama L, Shrestha S, Sharma A, Upadhyay S, Pathak MR. Immediate neonatal outcome of adolescent pregnant mother at Nepal Medical College Teaching Hospital. Nepal Med Coll J 2013;15(2):117-121PubMed
- 23. United Nations Children’s Fund (UNICEF). Adolescent health and well-being: ensuring their development and growth, with implications that reverberate across generations [cited 2023 Mar 1]. Available from: https://www.unicef.org/health/adolescent-health-and-well-being
- 24. International Institute for Population Science, ICF. National Family Health Survey (NFHS-4), 2015-16; 2017 [cited 2022 Sep 5]. Available from: https://dhsprogram.com/pubs/pdf/fr339/fr339.pdf
- 25. Gurung R, Målqvist M, Hong Z, Poudel PG, Sunny AK, Sharma S, et al. The burden of adolescent motherhood and health consequences in Nepal. BMC Pregnancy Childbirth 2020;20(1):318. https://doi.org/10.1186/s12884-020-03013-8ArticlePubMedPMC
- 26. World Health Organization. Adolescent pregnancy; 2022 [cited 2022 Mar 8]. Available from: https://www.who.int/newsroom/fact-sheets/detail/adolescent-pregnancy
- 27. Bhatta K, Bhandary S. Factors associated with adolescent pregnancy in selected rural municipalities of Lalitpur district: a mixed method study. J Gen Pract Emerg Med Nepal 2022;9(13):17-22. https://doi.org/10.59284/jgpeman39Article
- 28. Yakubu I, Salisu WJ. Determinants of adolescent pregnancy in sub-Saharan Africa: a systematic review. Reprod Health 2018;15(1):15. https://doi.org/10.1186/s12978-018-0460-4ArticlePubMedPMC
- 29. Fonner VA, Armstrong KS, Kennedy CE, O’Reilly KR, Sweat MD. School based sex education and HIV prevention in low- and middle-income countries: a systematic review and meta-analysis. PLoS One 2014;9(3):e89692. doi: https://doi.org/10.1371/journal.pone.0089692ArticlePubMedPMC
- 30. Donkor AK, Lariba AL. The impact of sex education on teenage pregnancy in basic schools of Bawku municipal district in Ghana. Indones J Biol Educ 2017;3(3):214-221. https://files.eric.ed.gov/fulltext/ED580282.pdfArticlePDF
- 31. Mark ND, Wu LL. More comprehensive sex education reduced teen births: quasi-experimental evidence. Proc Natl Acad Sci U S A 2022;119(8):e2113144119. https://doi.org/10.1073/pnas.2113144119ArticlePubMedPMC
- 32. Kohler PK, Manhart LE, Lafferty WE. Abstinence-only and comprehensive sex education and the initiation of sexual activity and teen pregnancy. J Adolesc Health 2008;42(4):344-351. https://doi.org/10.1016/j.jadohealth.2007.08.026ArticlePubMed
- 33. Oettinger GS. The effects of sex education on teen sexual activity and teen pregnancy. J Polit Econ 1999;107(3):606-644. https://doi.org/10.1086/250073Article
- 34. Sabia JJ. Does sex education affect adolescent sexual behaviors and health? J Policy Anal Manage 2006;25(4):783-802. https://doi.org/10.1002/pam.20208ArticlePubMed
- 35. Gautam L, Gupta A, Khadka R, Pant GP. A study to assess contributing factors of teenage pregnancy in Sunsari district of Nepal. Ind J Youth Adol Health 2020;7(2):5-11. https://doi.org/10.24321/2349.2880.202007Article
- 36. Bhandari SD. Awareness on consequences of teenage pregnancy among adolescent at Ampipal VDC, Gorkha. J Adv Acad Res 2014;1(1):10-17. https://doi.org/10.3126/jaar.v1i1.13506Article
- 37. Ramanadin PV, Sijo ME, Laxmanbhai IC, Manjibhai ML, Lasyabhai ML, Laxman MR, et al. A descriptive study to assess the knowledge on teenage pregnancy and its prevention among the teenage girl residing in selected areas of Dadra and Nagar Haveli. Int J Nurs Educ Res 2017;5(3):293-296. https://doi.org/10.5958/2454-2660.2017.00060.6Article
- 38. Manjula P, Sreelatha M, Sudharani P. A study to assess the knowledge of adolescent girls towards teenage pregnancy at selected government junior colleges, Tirupathi. Community Public Health Nurs 2016;1(2):89-94. https://doi.org/10.21088/cphn.2455.8621.1216.4Article
REFERENCES
Figure & Data
References
Citations
- Letter to the Editor: Teenage Pregnancy in the Philippines: Effects and Interventions
Dalmacito A. Cordero
Journal of Preventive Medicine and Public Health.2024; 57(3): 304. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite