Articles
- Page Path
- HOME > J Prev Med Public Health > Volume 55(4); 2022 > Article
-
Original Article
The Busan Regional CardioCerebroVascular Center Project’s Experience Over a Decade in the Treatment of ST-segment Elevation Myocardial Infarction -
Kyunghee Lim1
 , Hyeyeon Moon2, Jong Sung Park1, Young-Rak Cho1, Kyungil Park1, Tae-Ho Park1, Moo-Hyun Kim1, Young-Dae Kim1
, Hyeyeon Moon2, Jong Sung Park1, Young-Rak Cho1, Kyungil Park1, Tae-Ho Park1, Moo-Hyun Kim1, Young-Dae Kim1 -
Journal of Preventive Medicine and Public Health 2022;55(4):351-359.
DOI: https://doi.org/10.3961/jpmph.22.071
Published online: June 24, 2022
1Department of Cardiology, Busan Regional CardioCerebroVascular Center, Dong-A University Hospital, Busan, Korea
2Department of Endocrinology, Dong-A University Hospital, Busan, Korea
- Corresponding author: Jong Sung Park, Department of Cardiology, Busan Regional CardioCerebroVascular Center, Dong-A University Hospital, 32 Daesingonwon-ro, Seo-gu, Busan 49202, Korea, E-mail: thinkmed@dau.ac.kr
Copyright © 2022 The Korean Society for Preventive Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Objectives
- The Regional CardioCerebroVascular Center (RCCVC) project was initiated to improve clinical outcomes for patients with acute myocardial infarction or stroke in non-capital areas of Korea. The purpose of this study was to evaluate the outcomes and issues identified by the Busan RCCVC project in the treatment of ST-segment elevation myocardial infarction (STEMI).
-
Methods
- Among the patients who were registered in the Korean Registry of Acute Myocardial Infarction for the RCCVC project between 2007 and 2019, those who underwent percutaneous coronary intervention (PCI) for STEMI at the Busan RCCVC were selected, and their medical data were compared with a historical cohort.
-
Results
- In total, 1161 patients were selected for the analysis. Ten years after the implementation of the Busan RCCVC project, the median door-to-balloon time was reduced from 86 (interquartile range [IQR], 64–116) to 54 (IQR, 44–61) minutes, and the median symptom-to-balloon time was reduced from 256 (IQR, 180–407) to 189 (IQR, 118–305) minutes (p<0.001). Inversely, the false-positive PCI team activation rate increased from 0.6% to 21.4% (p<0.001). However, the 1-year cardiovascular death and major adverse cardiac event rates did not change. Even after 10 years, approximately 75% of the patients had a symptom-to-balloon time over 120 minutes, and approximately 50% of the patients underwent inter-hospital transfer for primary PCI.
-
Conclusions
- A decade after the implementation of the Busan RCCVC project, although time parameters for early reperfusion therapy for STEMI improved, at the cost of an increased false-positive PCI team activation rate, survival outcomes were unchanged.
- Keywords: Acute myocardial infarction, Percutaneous coronary intervention, Korea
- The Regional CardioCerebroVascular Center (RCCVC) project was initiated by the Ministry of Health and Welfare of Korea to improve clinical outcomes in the acute phase of treatment and to construct dedicated medical infrastructure for patients with cardiovascular or cerebrovascular diseases in non-capital areas of Korea [1]. One of the most important purposes of the RCCVC project was to establish an organized medical system that could provide early reperfusion therapy for patients with acute myocardial or cerebral infarction. Under the guidance of a special law for the RCCVC project launched in 2008, the country, excluding Seoul, was divided into 9 regions (12 regions in 2021), and a major tertiary hospital in each region was designated as an RCCVC [1]. Each RCCVC consists of cardiovascular, cerebrovascular, cardiocerebral rehabilitation, and prevention and management centers, which provide primary and secondary prevention services for acute ischemic heart and brain diseases.
- Dong-A University Hospital was assigned to the Busan RCCVC in June 2010. By adopting multiple strategies for early reperfusion therapy, the Busan RCCVC could reduce the door-to-balloon time; however, this reduction did not lead to an improvement in survival outcomes. The absence of a significant reduction in the symptom-to-balloon time was thought to be the main reason for the lack of improvement in survival outcomes [2]. The Community-Based Pre-Hospital Electrocardiogram Transmission Project for patients with ST-segment elevation myocardial infarction (STEMI) was conducted to reduce the first medical contact to balloon (FMC-to-balloon) time by directly transporting patients to the nearest percutaneous coronary intervention (PCI)-capable hospital and early activation of the PCI team [3]. However, upon completion of the Pre-Hospital Electrocardiogram Transmission project, the FMC-to-balloon time was prolonged, and the proportion of STEMI patients who were transferred to Busan RCCVC via PCI-incapable hospitals increased to the previous levels. In addition, there was concern regarding the marked increase in the rate of false-positive activation of the PCI team.
- We conducted this retrospective study to investigate temporal changes in clinical outcomes a decade after the implementation of the Busan RCCVC project in the treatment of STEMI and to identify problems caused by the project in order to determine future directions.
INTRODUCTION
- Study Population and Data Collection
- Patients who underwent emergency coronary angiography for suspected STEMI at the Busan RCCVC between June 2007 and May 2019 were screened. Patients for whom the clinical outcomes were not evaluable or the final diagnosis was not STEMI were excluded. The medical records of patients were extracted from the Korean Registry of Acute Myocardial Infarction (KRAMI), which is the main registry for evaluating the regional status of patients with acute coronary syndrome and the performance of each RCCVC [4]. Details regarding the registry have been published previously [4]. Additional data that could not be obtained from the KRAMI registry were collected from the institutional medical records. All medical records were reviewed by 2 cardiologists, and the data integrity was confirmed by an independent cardiologist.
- Evaluation of Clinical Outcomes and Problems
- The performance of the Busan RCCVC in providing early reperfusion therapy was evaluated using 3 major reperfusion time indexes (door-to-balloon, symptom-to-balloon, and FMC-to-balloon time). The FMC time was defined as the time point when 119 (the emergency number in Korea) emergency medical system (EMS) personnel contacted the patient or the patient arrived at the emergency department during the first hospital visit.
- Cardiovascular death and major adverse cardiac events (MACEs) within 1 year after the index event were used to assess the survival outcomes. MACEs were defined as the composite of total cardiovascular death, non-fatal myocardial infarction, congestive heart failure, unplanned revascularization, and major bleeding.
- We also identified cases with false-positive PCI team activation and evaluated which types of abnormal electrocardiogram (ECG) findings were misinterpreted as STEMI in those cases. The criteria for ST-segment elevation in 12-lead ECG were adopted from the fourth Universal Definition of Myocardial Infarction [5]. Acute total or near-total occlusions, intravascular thrombus, or luminal narrowing of >75% that required emergent PCI or coronary artery bypass graft (CABG) on diagnostic coronary angiography were defined as culprit lesions. False-positive PCI team activation was defined as the absence of a culprit lesion on diagnostic coronary angiography.
- Statistical Analysis
- Patients who visited the Busan RCCVC during the 3 years prior to the project initiation (June 1, 2007 to May 31, 2010) were selected as the historical cohort and defined as the control group. All patients who visited the center 9 years after the project initiation (June 1, 2010 to May 31, 2019) were defined as the project group. We divided the entire project period of 9 years into 3 periods (control: June 1, 2007 to May 31, 2010; period 1: June 1, 2010 to May 31, 2013; period 2: June 1, 2013 to May 31, 2016; period 3: June 1, 2016 to May 31, 2019). We examined temporal changes in clinical outcomes and false-positive PCI team activation rates between the control and project groups and analyzed them according to the periods.
- The patients who were transported to the Busan RCCVC by the 119 EMS team without passing through PCI-incapable hospitals or who visited the center on their own or by public transport were included in the direct transport/visit group. Patients who were transferred from PCI-incapable hospitals to the Busan RCCVC for primary reperfusion therapy were defined as the inter-hospital transfer group. Temporal changes in the proportion of the inter-hospital transfer group and the different reperfusion time indexes between the two groups were compared according to the periods.
- The values of all continuous variables are presented as medians with interquartile ranges (IQRs), and the independent t-test was performed to compare continuous variables. In addition, four independent groups were compared using 1-way analysis of variance or the Welch test according to homoscedasticity, followed by post hoc analysis (Bonferroni or Games-Howell test). Categorical variables were presented as numbers and percentages (%), and the chi-square test was performed to compare the differences between the variables. Cardiovascular deaths and the incidence of MACEs after project initiation were evaluated using the Kaplan–Meier method, and intergroup comparisons were performed using the log-rank test. Differences were considered statistically significant when the p-value was ≤0.05. All statistical analyses were performed using SPSS version 20.0 (IBM Corp., Armonk, NY, USA).
- Ethics Statement
- This study was conducted after receiving full review and approval from the Institutional Review Board of Dong-A University Hospital (IRB No. DAUHIRB-20-111). Written informed consent was routinely obtained from patients before discharge.
METHODS
- Study Population
- The number of patients who underwent coronary angiography for suspected STEMI from June 1, 2007 to May 31, 2019, was 1560. Patients who died before coronary angiography (n=14), chose not to receive PCI (n=4), visited the emergency department without ongoing symptoms or signs of myocardial ischemia 6 hours after the onset of chest pain (n=127), and had deferred due to spontaneous resolution of both chest pain and ST-segment elevation (n=30) were excluded. We also excluded cases with false-positive PCI team activation (n=224). A total of 1161 patients were finally selected for analysis. There were 909 male (78.3%), and the median age of all patients was 63 years (IQR, 54–74). The percentage of patients aged ≥80 years was 10.6% in the control period and 11.5%, 12.6%, and 15.0% in each subsequent period (p=0.023). Nine patients underwent fibrinolysis, and 12 patients underwent CABG. When the study population was divided into a control group (n=180) and a project group (n=981), the project group was predominantly male and had a higher prevalence of dyslipidemia than the control group. The systolic and diastolic blood pressure in the control group were lower than those of the project group, but were within the normal range in both groups. The demographic and clinical characteristics of the STEMI patients are presented in Table 1 and Supplemental Material 1.
- Temporal Changes of Reperfusion Time Indexes
- After the implementation of the Busan RCCVC project, the median values of door-to-balloon and symptom-to-balloon times decreased from 86 (IQR, 64–116) and 256 (IQR, 180–407) minutes to 54 (IQR, 44–61) and 189 (IQR, 118–305) minutes, respectively (p<0.001). The FMC-to-balloon time was identified in 948 (82%) patients, and the median FMC-to-balloon time was reduced from 134 (IQR, 85–188) to 81 (IQR, 54–140) minutes (p<0.001). Patients who underwent CABG were excluded from the analysis when evaluating the reperfusion time indexes. Although the median values of door-to-balloon and symptom-to-balloon times decreased rapidly and consistently during period 1, little change was observed in those indexes in periods 2 and 3 (Figure 1A). The percentage of patients with door-to-balloon time <60 minutes and symptom-to-balloon time <120 minutes increased from 20.2% and 4.9% to 80.2% and 26.2%, respectively (Figure 1B). The percentage of patients with FMC-to-balloon time <90 minutes also increased from 31.1% to 55.6% (Figure 1B). Temporal changes in reperfusion time indexes are presented in Table 1 and Figure 1.
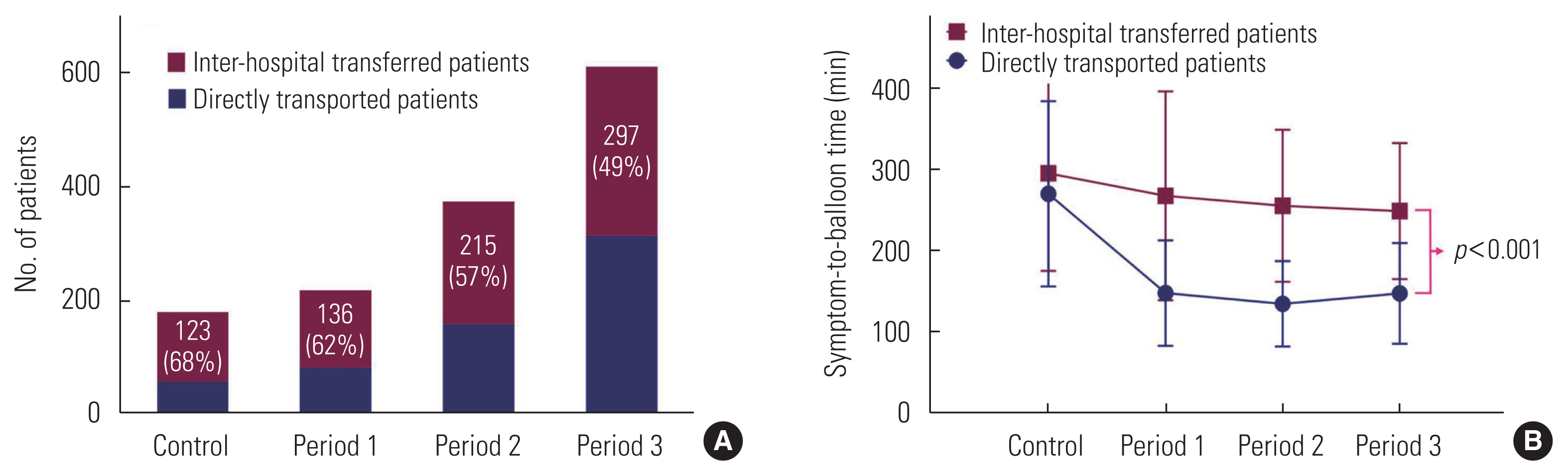
- Temporal Changes in the Inter-hospital Transfer Rate
- The study population was divided into the direct transport/visit group (n=390) and the inter-hospital transfer group (n= 771). The absolute number of patients who underwent inter-hospital transfer increased from 123 to 297 despite the decrease in the percentage of patients who were transferred from PCI-incapable hospitals (from 68 to 49%) (Figure 2A). Although the median door-to-balloon time did not significantly differ between the inter-hospital transfer group and the direct transport/visit group (55 [IQR, 45–60] vs. 56 [IQR, 44–66] minutes, respectively, p=0.089), the median symptom-to-balloon time (247 [IQR, 174–356] vs. 135 [IQR, 97–223] minutes, p<0.001) was significantly longer in the inter-hospital transfer group. The symptom-to-balloon time was significantly reduced in the direct transport/visit group, but not in the inter-hospital transfer group (p<0.001) (Figure 2B). In the inter-hospital transfer group, 27–50% of the patients were transferred from local PCI-incapable hospitals (Supplemental Material 1), which were in locations other than those assigned within the scope of the Busan RCCVC (eastern Gyeongnam Province). These patients had longer median FMC-to-balloon times than those transferred from local PCI-incapable hospitals within the scope of the Busan RCCVC (152 [IQR, 131–188] vs. 137 [IQR, 105–189] minutes, p=0.001). However, there was no significant inter-group differences in the symptom-to-balloon time (260 [IQR, 171–372] vs. 238 [IQR, 170–360] minutes, p=0.535) (analysis results not shown in the Figures).
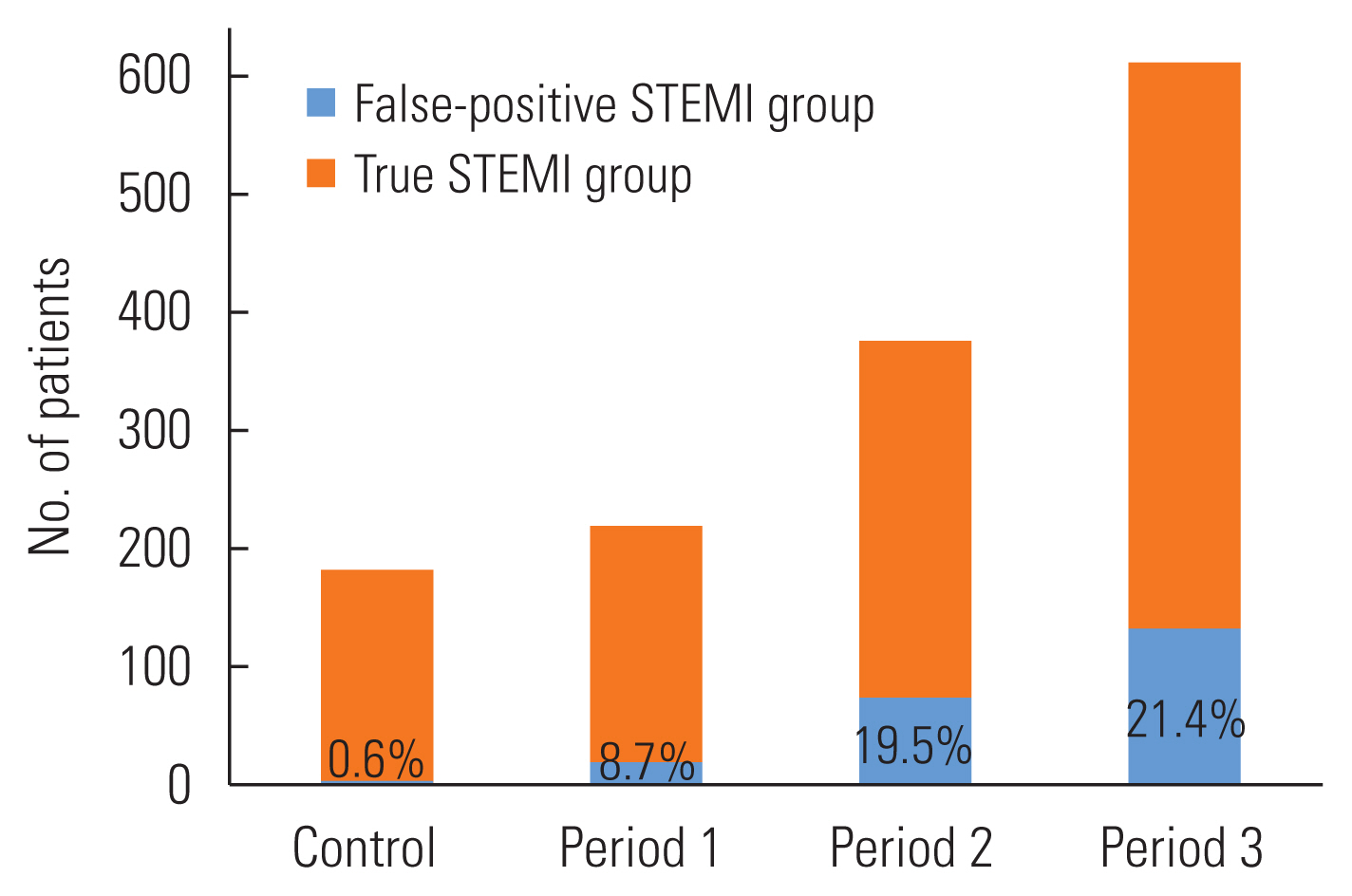
- Temporal Changes in the False-positive Percutaneous Coronary Intervention Team Activation Rate
- The total number of cases with false-positive PCI team activation was 224 (16.1%). In contrast to the control group (0.6%), the false-positive PCI team activation rate in the project group drastically increased to 21.4% in period 3 (Figure 3). ECG abnormalities can be largely classified into 3 groups: structural heart disease, non-structural (electrical) heart disease, and others, including vasospastic angina. Pre-existing ST-segment elevations, which were misinterpreted as new-onset ST-segment elevations in patients with ischemic or other structural heart diseases, accounted for the largest proportion of false-positive activations (n=36), followed by vasospastic angina (n=33), stress-induced cardiomyopathy (n=29), myocarditis or pericarditis (n=27), early repolarization (n=12), and bundle branch block (n=8). The ECG abnormalities that led to the misdiagnosis of STEMI are summarized in Supplemental Material 2.
- Temporal Changes in Survival Outcomes
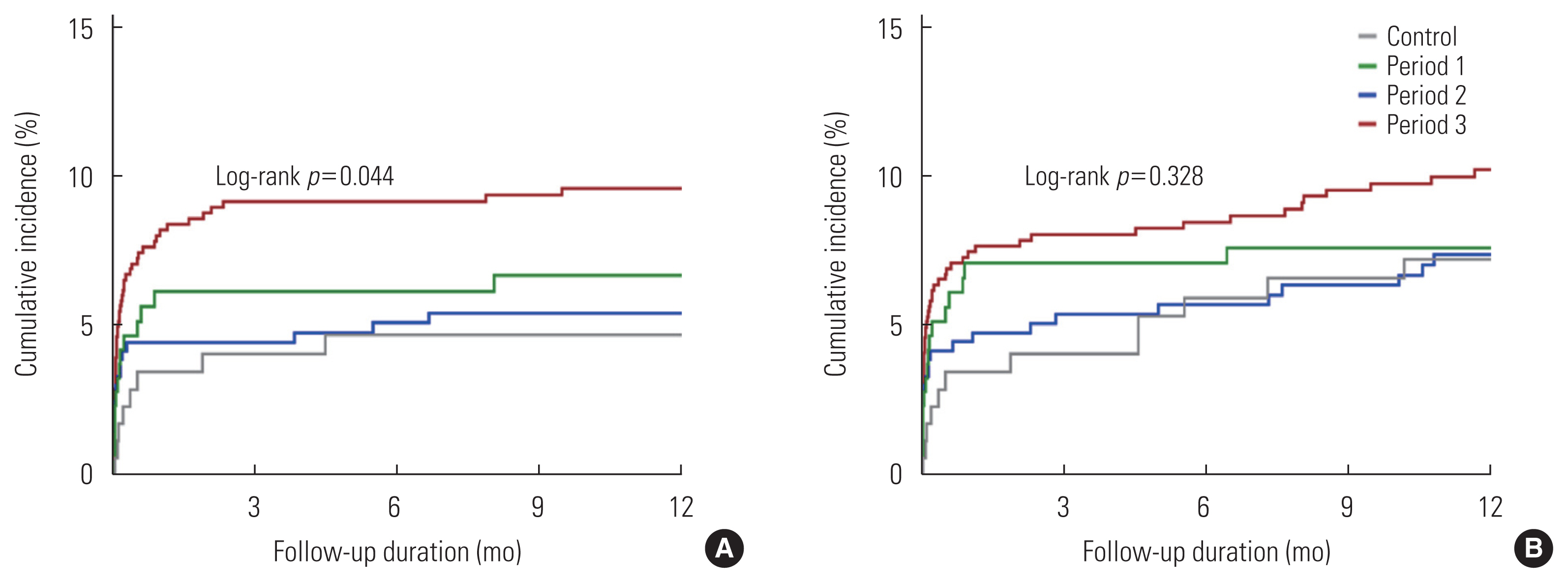
- The cumulative incidence of cardiovascular death within 1 year after STEMI was 5.0% in the control period and 8.5%, 5.6%, and 10.6% in each period, with a significant increase in period 3 (Figure 4A). The cumulative incidence of MACEs within 1 year after STEMI was 12.7% in the control period and 13.7%, 13.1%, and 16.2% in each period, with similar but insignificant increases in period 3 (Figure 4B). The percentages of patients with cardiogenic shock at the time of initial presentation were 25.0% in the control period and 39.5%, 26.2%, and 44.6% in each period (p<0.001) (Supplemental Material 1).
RESULTS
- This study was conducted to evaluate the clinical outcomes and issues before and after the implementation of the Busan RCCVC project. The findings can be summarized as follows: first, all reperfusion time indexes had the greatest improvement in the first period. Second, although the proportion of patients who were transferred from a PCI-incapable hospital tended to decrease, it remained high at about 50% until the final period, and the symptom-to-balloon time in the inter-hospital transfer group did not decrease. Third, the false-positive PCI team activation rate continued to be elevated, exceeding 20% in the final period. Fourth, the cardiovascular death and MACE rates did not decrease over the decade after the implementation of the Busan RCCVC project.
- The results of the Busan RCCVC project, which was conducted by the government, suggest that it takes approximately 3 years for an early reperfusion treatment policy in patients with STEMI to be established. During the project period, the door-to-balloon time was maintained within 60 minutes [6], which is similar to that of the Korea Acute Myocardial Infarction Registry data released in 2019 [7]. After the implementation of the Busan RCCVC project, the cardiovascular death and MACE rates within 1 year did not decrease despite a reduction in the symptom-to-balloon time from 256 minutes to 189 minutes. Failure to reduce the symptom-to-balloon time to <120 minutes, which is the goal of early reperfusion therapy recommended by the guidelines of major cardiology societies [8,9], seems to be the major reason why cardiovascular death and MACE rates did not decrease. The symptom-to-balloon time is an important reperfusion time index that closely correlates with the extent of transmural necrosis and the mortality of patients with STEMI [10–12]. In the present study, approximately 75% of the patients had a symptom-to-balloon time of >120 minutes, even in the final period. The insufficient reduction in the symptom-to-balloon time can be explained by the high inter-hospital transfer rate. Inter-hospital transfer is known to be a major risk factor for prolonging the symptom-to-balloon time [13–15]. In this study, the symptom-to-balloon time in the inter-hospital transfer group was significantly longer than that of the direct transport/visit group, and the symptom-to-balloon time was reduced only in the direct transport/visit group after the project. Although the proportion of patients who belonged to the inter-hospital transfer group gradually decreased, approximately 50% of the patients underwent inter-hospital transfer for primary PCI, even in the final period. The highest cardiovascular death and MACE rates occurred in period 3, which can be explained by the higher percentage of octogenarians (15.0%) and patients with cardiogenic shock at the time of initial presentation (44.6%) in that period. As Busan Metropolitan City is rapidly transforming into an aged society, survival outcomes seem likely to worsen in the future.
- These results suggest that efforts to reduce the door-to-balloon time in each PCI-capable hospital do not impact survival outcomes in Korea. Efforts to create an organized early diagnosis and referral system that integrates the 119 EMS team for STEMI patients should be made by cardiology and emergency medicine societies in collaboration with regional fire and disaster headquarters. For pre-hospital ECG diagnosis and triage, which are essential in bypassing PCI-incapable hospitals, political and legal support for the participation of 119 EMS personnel in the system will be important.
- Primary PCI is the preferred reperfusion strategy for STEMI treatment [6]. Considering that the main purpose of the RCCVC project was to provide early reperfusion therapy, an increase in the rate of false-positive PCI team activation is inevitable to some extent. The policy of the Ministry of Health and Welfare of Korea to unequally allocate project budgets depending on each RCCVC’s performance might have induced excessive competition between participating centers to improve reperfusion time indexes. In previous prospective studies, rates of false-positive PCI team activation ranged from 7.5% to 14.6% [16–18]. However, in this study, the false-positive PCI team activation rate increased to 21.4% in the final period. A certain level of false-positive PCI team activation is essential to ensure adequate sensitivity for the early diagnosis of STEMI [19]. However, excessive false-positive activation may exhaust medical staff, thus reducing the procedural quality of PCI. Maintaining a false-positive PCI team activation rate at an appropriate level, which can be tolerated by medical staff without reducing the diagnostic sensitivity, is important, especially in the long term. Therefore, it is plausible that patients with a history of ischemic heart disease, such as previous myocardial infarction, may be frequently misdiagnosed as having STEMI, and a more difficult diagnostic algorithm might be suggested for these patients. Detailed history-taking and ECG inspection, as well as bedside echocardiography, would have discriminated false STEMI in a large number of cases.
- This study has several major limitations. First, the results do not reflect the general circumstances of the 12 RCCVCs in the country, as data were only collected from a single RCCVC. Unlike other centers, the Busan RCCVC covers a metropolitan city with several PCI-capable local hospitals. In addition, many patients are transferred from PCI-incapable hospitals in locations other than those assigned within the scope of the Busan RCCVC, as they may be geographically close to Busan Metropolitan City but administratively belong to the service area of another RCCVC. The geographic characteristics of the Busan RCCVC may have influenced the patients’ characteristics and clinical outcomes. Second, as a retrospective study using data collected from the KRAMI registry, the quality and quantity of extracted data are limited, making it difficult to confirm the causal relationship between variables. We were unable to collect some data, such as the exact FMC time or mode of transport/visit to the referring hospital, which were not included in the KRAMI registry. Third, differences in baseline characteristics between the control and project groups might have affected the survival outcomes such as cardiovascular death or MACE. Fourth, we cannot be sure whether the significant improvement in the time parameters for early reperfusion therapy were the direct results of the Busan RCCVC project. Medical infrastructure, including human resources and healthcare facilities in Busan Metropolitan City, was substantially expanded during the last decade. For example, the number of 119 EMS personnel in Busan Metropolitan City approximately doubled and the number of cardiology specialists at PCI-incapable hospitals increased significantly in the same period. Improvements in the time parameters for early reperfusion therapy may have been due to a combination of results from the Busan RCCVC project and the improved status of medical infrastructure in Busan Metropolitan City. To better understand the outcomes of the RCCVC project, further studies should compare the performance of RCCVCs and other cardiovascular centers that did not participate in the RCCVC project. Our findings should be interpreted cautiously considering the above limitations.
- After the implementation of the Busan RCCVC project, the door-to-balloon, symptom-to-balloon, and FMC-to-balloon times consistently decreased. However, these improvements in the reperfusion time indexes did not translate to a reduction in cardiovascular death and MACE rates. Conversely, as a consequence of the improved reperfusion time indexes, the false-positive PCI team activation rate considerably increased. Even in the final period, a large proportion of patients still underwent inter-hospital transfers for primary PCI. Future policy initiatives for the RCCVC project should focus on further reduction of the symptom-to-balloon time, which can be achieved by minimizing unnecessary inter-hospital transfers.
DISCUSSION
SUPPLEMENTAL MATERIALS
-
CONFLICT OF INTEREST
The authors have no conflicts of interest associated with the material presented in this paper.
-
FUNDING
This study was funded by the Research Fund of Dong-A University.
Notes
ACKNOWLEDGEMENTS
-
AUTHOR CONTRIBUTIONS
Conceptualization: Lim K, Park JS. Data curation: Lim K, Moon H, Park JS. Formal analysis: Lee K, Moon H, Park JS. Funding acquisition: Park JS. Methodology: Lim K, Moon H, Park JS, Cho YR, Park K, Park TH, Kim MH, Kim YD. Writing – original draft: Lim K. Writing – review & editing: Lim K, Moon H, Park JS, Cho YR, Park K, Park TH, Kim MH, Kim YD.
Notes


| Characteristics | Control (n=180) | Project (n=981) | p-value1 |
|---|---|---|---|
| Sex, male | 126 (70.0) | 783 (79.8) | 0.0032 |
|
|
|||
| Age (y) | 62 [53–72] | 63 [54–74] | 0.262 |
|
|
|||
| Body mass index (kg/m2) | 23.5 [21.5–25.3] | 23.9 [22.0–25.7] | 0.167 |
|
|
|||
| Systolic blood pressure (mmHg) | 110 [100–130] | 120 [105–134] | <0.001 |
|
|
|||
| Diastolic blood pressure (mmHg) | 70 [60–80] | 70 [62–80] | 0.004 |
|
|
|||
| Previous PCI | 22 (12.2) | 118 (12.0) | 0.942 |
|
|
|||
| Prior myocardial infarction | 19 (10.6) | 104 (10.6) | 0.985 |
|
|
|||
| Comorbid diseases | |||
| Hypertension | 92 (51.1) | 519 (52.9) | 0.658 |
| Diabetes mellitus | 66 (36.7) | 352 (35.9) | 0.840 |
| Dyslipidemia | 16 (8.9) | 363 (37.0) | <0.001 |
| Smoking | 93 (51.7) | 458 (46.7) | 0.230 |
| Prior stroke | 12 (6.7) | 99 (10.1) | 0.151 |
| COPD/bronchial asthma | 7 (3.9) | 32 (3.3) | 0.668 |
| Chronic kidney disease, stage 4–5 | 5 (2.8) | 39 (4.0) | 0.439 |
|
|
|||
| Symptom-to-balloon time (min) | 256 [180–407] | 189 [118–305] | <0.001 |
|
|
|||
| Door-to-balloon time (min) | 86 [64–116] | 54 [44–61] | <0.001 |
|
|
|||
| FMC-to-balloon time (min) | 134 [85–188] | 81 [54–140] | <0.001 |
|
|
|||
| Location of referral hospital | <0.001 | ||
| Busan Metropolitan City | 90 (50.0) | 398 (40.6) | |
| Gyeongnam Province | 33 (18.3) | 250 (25.5) | |
|
|
|||
| Culprit artery | 0.394 | ||
| Left main | 1 (0.6) | 27 (2.8) | |
| Left anterior descending | 97 (53.9) | 533 (54.3) | |
| Left circumflex | 15 (8.3) | 93 (9.5) | |
| Right coronary | 67 (37.2) | 328 (33.4) | |
|
|
|||
| Cardiogenic shock | 45 (25.0) | 372 (37.9) | <0.001 |
|
|
|||
| ECMO | 6 (3.3) | 29 (3.0) | 0.786 |
|
|
|||
| CCU admission duration (day) | 3 [2–4] | 3 [2–4] | 0.160 |
|
|
|||
| LVEF at discharge (%) | 47.5 [42.5–52.0] | 47.0 [42.5–57.3] | 0.737 |
|
|
|||
| LVEF ≤35% at discharge | 15 (8.3) | 66 (6.7) | 0.500 |
|
|
|||
| LV end diastolic dimension (mm) | 48 [45–51] | 49 [46–50] | 0.156 |
|
|
|||
| Survival discharge rate (%) | 168 (93.3) | 897 (91.4) | 0.331 |
|
|
|||
| Survival rate at 1 y (%) | 167 (92.8) | 887 (90.4) | 0.226 |
Values are presented as number (%) or median [interquartile range].
PCI, percutaneous coronary intervention; COPD, chronic obstructive lung disease; FMC, first medical contact; ECMO, extracorporeal membrane oxygenation; CCU, coronary care unit; LVEF, left ventricular ejection fraction; LV, left ventricular.
1 The p-value denotes statistical significance comparing the control group and project group.
2 Calculated by the independent t-test or chi-square test.
- 1. Korean Ministry of Health and Welfare. Guide for regional cardiocerebro vascular center project. Seoul: Ministry of Health and Welfare; 2008. p. 5-6 (Korean)
- 2. Lee DH, Seo JM, Choi JH, Cho YR, Park K, Park TH, et al. Early experience of Busan-Ulsan regional cardiocerebrovascular center project in the treatment of ST elevation myocardial infarction. Korean J Med 2013;85(3):275-284. (Korean)Article
- 3. Park K, Park JS, Cho YR, Park TH, Kim MH, Yang TH, et al. Community-based pre-hospital electrocardiogram transmission program for reducing systemic time delay in acute ST-segment elevation myocardial infarction. Korean Circ J 2020;50(8):709-719ArticlePubMedPMCPDF
- 4. Kim RB, Hwang JY, Park HW, Her AY, Lee JH, Kim MH, et al. Contemporary status of acute myocardial infarction in Korean patients: Korean registry of acute myocardial infarction for regional cardiocerebrovascular centers. J Clin Med 2021;10(3):498ArticlePubMedPMC
- 5. Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, et al. Fourth universal definition of myocardial infarction (2018). Circulation 2018;138(20):e618-e651ArticlePubMed
- 6. Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J 2018;39(2):119-177PubMed
- 7. Kim Y, Ahn Y, Cho MC, Kim CJ, Kim YJ, Jeong MH. Current status of acute myocardial infarction in Korea. Korean J Intern Med 2019;34(1):1-10ArticlePubMedPMCPDF
- 8. Antman EM, Hand M, Armstrong PW, Bates ER, Green LA, Halasyamani LK, et al. 2007 focused update of the ACC/AHA 2004 guidelines for the management of patients with ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the Canadian Cardiovascular Society endorsed by the American Academy of Family Physicians: 2007 writing group to review new evidence and update the ACC/AHA 2004 guidelines for the management of patients with ST-elevation myocardial infarction, writing on behalf of the 2004 writing committee. Circulation 2008;117(2):296-329ArticlePubMed
- 9. Denktas AE, Anderson HV, McCarthy J, Smalling RW. Total ischemic time: the correct focus of attention for optimal ST-segment elevation myocardial infarction care. JACC Cardiovasc Interv 2011;4(6):599-604PubMed
- 10. Khalid U, Jneid H, Denktas AE. The relationship between total ischemic time and mortality in patients with STEMI: every second counts. Cardiovasc Diagn Ther 2017;7(Suppl 2):S119-S124ArticlePubMedPMC
- 11. Greulich S, Mayr A, Gloekler S, Seitz A, Birkmeier S, Schäufele T, et al. Time-dependent myocardial necrosis in patients with ST-segment-elevation myocardial infarction without angiographic collateral flow visualized by cardiac magnetic resonance imaging: results from the multicenter STEMI-SCAR project. J Am Heart Assoc 2019;8(12):e012429ArticlePubMedPMC
- 12. Kim HK, Jeong MH, Ahn Y, Chae SC, Kim YJ, Hur SH, et al. Relationship between time to treatment and mortality among patients undergoing primary percutaneous coronary intervention according to Korea Acute Myocardial Infarction Registry. J Cardiol 2017;69(1):377-382ArticlePubMed
- 13. Langabeer JR 2nd, Prasad S, Seo M, Smith DT, Segrest W, Owan T, et al. The effect of interhospital transfers, emergency medical services, and distance on ischemic time in a rural ST-elevation myocardial infarction system of care. Am J Emerg Med 2015;33(7):913-916ArticlePubMed
- 14. Kawecki D, Gierlotka M, Morawiec B, Hawranek M, Tajstra M, Skrzypek M, et al. Direct admission versus interhospital transfer for primary percutaneous coronary intervention in ST-segment elevation myocardial infarction. JACC Cardiovasc Interv 2017;10(5):438-447ArticlePubMed
- 15. De Luca G, Suryapranata H, Ottervanger JP, Antman EM. Time delay to treatment and mortality in primary angioplasty for acute myocardial infarction: every minute of delay counts. Circulation 2004;109(10):1223-1225ArticlePubMed
- 16. Bae MH, Cheon SS, Song JH, Jang SY, Choi WS, Kim KH, et al. Etiologies and predictors of ST-segment elevation myocardial infarction. Korean Circ J 2013;43(6):370-376ArticlePubMedPMC
- 17. Nfor T, Kostopoulos L, Hashim H, Jan MF, Gupta A, Bajwa T, et al. Identifying false-positive ST-elevation myocardial infarction in emergency department patients. J Emerg Med 2012;43(4):561-567ArticlePubMed
- 18. Regueiro A, Fernández-Rodríguez D, Freixa X, Bosch X, Martín-Yuste V, Brugaletta S, et al. False positive STEMI activations in a regional network: comprehensive analysis and clinical impact. Results from the Catalonian codi infart network. Rev Esp Cardiol (Engl Ed) 2018;71(4):243-249ArticlePubMed
- 19. McCabe JM, Armstrong EJ, Kulkarni A, Hoffmayer KS, Bhave PD, Garg S, et al. Prevalence and factors associated with false-positive ST-segment elevation myocardial infarction diagnoses at primary percutaneous coronary intervention–capable centers: a report from the Activate-SF registry. Arch Intern Med 2012;172(11):864-871PubMed
REFERENCES
Figure & Data
References
Citations
- Trends in Regional Disparities in Cardiovascular Surgery and Mortality in Korea: A National Cross-sectional Study
Dal-Lae Jin, Kyoung-Hoon Kim, Euy Suk Chung, Seok-Jun Yoon
Journal of Preventive Medicine and Public Health.2024; 57(3): 260. CrossRef - Mortality and Disparities of Acute Myocardial Infarction and Stroke in Korea, 2008–2019
Ji-Sook Choi, Soomin Kim, Choon-Seon Park, Hyejin Lee, Jin Yong Lee, Sun Min Kim
Yonsei Medical Journal.2024;[Epub] CrossRef - Relevance Index Regional Variation by Each Disease and Its Essential Medical Field: A Retrospective Data Analysis From 2016-2020 in Korea
Young-Eun Kim, Jeehee Pyo, Haneul Lee, HyeRan Jeong, Young-Kwon Park, Jeong-Wook Seo, Minsu Ock, Seok-Jun Yoon
Journal of Korean Medical Science.2023;[Epub] CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite