Articles
- Page Path
- HOME > J Prev Med Public Health > Volume 44(3); 2011 > Article
-
Original Article
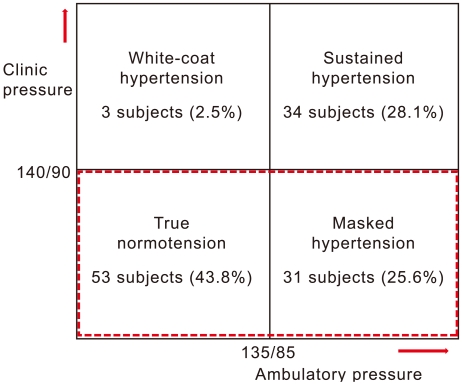
Frequency and Related Factors of Masked Hypertension at a Worksite in Korea - Sang-Kyu Kim1, Jun-Ho Bae2, Dung-Young Nah2, Dong-Wook Lee3, Tae-Yoon Hwang4, Kyeong-Soo Lee4
-
Journal of Preventive Medicine and Public Health 2011;44(3):131-139.
DOI: https://doi.org/10.3961/jpmph.2011.44.3.131
Published online: May 17, 2010
1Department of Preventive Medicine, Dongguk University College of Medicine, Gyeongju, Korea.
2Department of Internal Medicine, Dongguk University College of Medicine, Gyeongju, Korea.
3Department of Family Medicine, Dongguk University College of Medicine, Gyeongju, Korea.
4Department of Preventive Medicine and Public Health, Yeungnam University College of Medicine, Daegu, Korea.
- Corresponding author: Kyeong-Soo Lee, MD, PhD. 317-1, Daemyung-dong, Nam-gu, Daegu 705-717, Korea. Tel: +82-53-620-4373, Fax: +82-53-653-2061, drkslee@ynu.ac.kr
• Received: October 15, 2010 • Accepted: March 17, 2011
Copyright © 2011 The Korean Society for Preventive Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
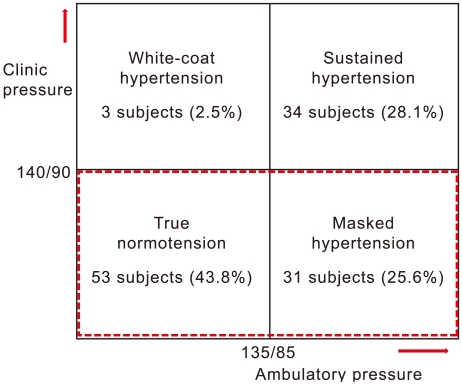
Figure & Data
References
Citations
Citations to this article as recorded by 
- Does This Adult Patient Have Hypertension?
Anthony J. Viera, Yuichiro Yano, Feng-Chang Lin, David L. Simel, Jonathan Yun, Gaurav Dave, Ann Von Holle, Laura A. Viera, Daichi Shimbo, Shakia T. Hardy, Katrina E. Donahue, Alan Hinderliter, Christiane E. Voisin, Daniel E. Jonas
JAMA.2021; 326(4): 339. CrossRef - Prevalence and determinants of masked hypertension among obese individuals at the Yaoundé Central Hospital: a cross-sectional study in sub-Saharan Africa
Bâ Hamadou, Sylvie Ndongo Amougou, Yolande Tchuendem, Chris Nadège Nganou-Gnindjio, Liliane Mfeukeu-Kuate, Audrey Joyce Foka, Aurel T. Tankeu, Ahmadou Musa Jingi, Alain Patrick Menanga, Samuel Kingue
Blood Pressure Monitoring.2020; 25(4): 212. CrossRef - Frequency of masked hypertension and its relation to target organ damage in the heart
Abdulsalam Mahmoud Algamal
The Egyptian Heart Journal.2016; 68(1): 53. CrossRef - Relationship between epistaxis and hypertension: A cause and effect or coincidence?
Nabil Abdulghany Sarhan, Abdulsalam Mahmoud Algamal
Journal of the Saudi Heart Association.2015; 27(2): 79. CrossRef - Blood pressure variability over 24 h: prognostic implications and treatment perspectives. An assessment using the smoothness index with telmisartan–amlodipine monotherapy and combination
Gianfranco Parati, Helmut Schumacher
Hypertension Research.2014; 37(3): 187. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite