
Articles
- Page Path
- HOME > J Prev Med Public Health > Volume 56(6); 2023 > Article
-
Original Article
Impact of Physical Activity on the Association Between Unhealthy Adolescent Behaviors and Anxiety Among Korean Adolescents: A Cross-sectional Study -
Hyo-jung Lee1
 , Jeong Pil Choi1, Kunhee Oh1, Jin-Young Min2, Kyoung-Bok Min1,3
, Jeong Pil Choi1, Kunhee Oh1, Jin-Young Min2, Kyoung-Bok Min1,3 -
Journal of Preventive Medicine and Public Health 2023;56(6):552-562.
DOI: https://doi.org/10.3961/jpmph.23.313
Published online: November 15, 2023
- 1,381 Views
- 104 Download
1Department of Preventive Medicine, Seoul National University College of Medicine, Seoul, Korea
2Veterans Medical Research Institute, Veterans Health Service Medical Center, Seoul, Korea
3Institute of Health Policy and Management, Medical Research Center, Seoul National University, Seoul, Korea
- Corresponding author: Kyoung-Bok Min, Department of Preventive Medicine, Seoul National University College of Medicine, 103 Daehak-ro, Jongno-gu, Seoul 03080, Korea E-mail: minkb@snu.ac.kr
Copyright © 2023 The Korean Society for Preventive Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Objectives
- Adolescents who engage in unhealthy behaviors are particularly vulnerable to anxiety. We hypothesized that participation in physical activity could influence the relationship between anxiety and unhealthy behaviors in adolescents. These behaviors include smoking, alcohol consumption, and unsafe sexual activity.
-
Methods
- This study included 50 301 students from the first year of middle school to the third year of high school, all from Korea. The unhealthy adolescent behaviors examined included current alcohol consumption, current smoking, and unsafe sexual behavior. Anxiety levels were assessed using the Generalized Anxiety Disorder-7 questionnaire (GAD-7).
-
Results
- The participants had a mean age of 15.19 years and an average GAD-7 score of 4.23. No significant differences were observed in GAD-7 score among exercising participants when categorized by smoking status (p=0.835) or unsafe sexual behavior (p=0.489). In contrast, participants in the non-exercise group who engaged in these behaviors demonstrated significantly higher GAD-7 scores (p<0.001 and 0.016, respectively). The only significant interaction was found between unsafe sexual behavior and exercise (p=0.009). Based on logistic regression analysis, within the non-exercise group, significant positive associations were observed between current smoking and anxiety (odds ratio [OR], 1.36; 95% confidence interval [CI], 1.18 to 1.57), as well as between unsafe sexual behavior and anxiety (OR, 1.33; 95% CI, 1.02 to 1.73). However, within the exercise group, no significant association was found between anxiety and either smoking or unsafe sexual behavior. Furthermore, no significant interaction was observed between unhealthy behaviors and exercise.
-
Conclusions
- These findings are insufficient to conclude that physical activity influences the relationship between unhealthy behaviors and anxiety.
- Adolescent health, including physical, mental, and social well-being, is of the utmost importance [1-5]. Tobacco and alcohol use persist as the most common risky behaviors among adolescents. As of 2017, 19.6% of high school students in the United States were current smokers, and current alcohol drinkers included 18.8% of male and 26.8% of female adolescents [6-9]. In Korea, the average age of first drinking experience has been steadily decreasing, from 13.0 years for boys and 13.7 years for girls in 2018, to 12.9 years for boys and 13.5 years for girls in 2019 [10]. Furthermore, early pregnancy and childbirth resulting from unsafe sexual behavior have been identified among the key adolescent health issues highlighted by the World Health Organization (WHO) and Sustainable Development Goal 3. In Africa, for example, despite a decline in the adolescent birth rate, the prevalence of teenage pregnancy remained high in 2020, at 25.4% [11].
- Adolescents engaging in unhealthy behaviors, including smoking, alcohol consumption, and risky sexual activities, frequently exhibit low self-efficacy. This renders them more susceptible to anxiety than their counterparts who do not engage in such behaviors [12-14]. The act of smoking cigarettes may incite anxiety via the manipulation of neurotransmitter systems and the induction of epigenetic alterations [15]. Comorbidities such as alcohol abuse and anxiety disorders are common [16], and ethanol may alter neurobiological mechanisms that modulate stress and anxiety circuits [17].
- Research has indicated that regular exercise can effectively reduce anxiety and its symptoms [18,19]. The positive impact of consistent exercise appears to be comparable to those of meditation or relaxation. Exercise can also enhance an individual’s self-efficacy, thereby reducing anxiety. Individuals with high self-efficacy report significantly lower anxiety levels after exercising compared to those with low self-efficacy [20].
- The relationship between unhealthy behaviors and anxiety, as well as between exercise and anxiety, has been well established. However, the dynamics of these relationships remain complex. Despite the rising prevalence of unhealthy behaviors among young people and the increasing recognition of the importance of physical activity, the specific impact of exercise and any potential interactions with unhealthy behaviors remain ambiguous. This study was conducted to explore the potential role of physical activity in relation to anxiety among adolescents engaging in unhealthy behaviors.
INTRODUCTION
- Study Population
- The Korea Youth Risk Behavior Survey is conducted to assess the health behaviors of Korean adolescents, plan and evaluate youth health promotion programs, and generate health indicators for international comparison [21]. Initiated in 2005, this annual survey is performed in accordance with government-approved statistics (Statistics Korea, approval No. 11758). The target demographic for the survey includes students from the first year of middle school through the third year of high school. The survey utilizes an anonymous, self-administered online questionnaire, with students participating via computer labs within their schools.
- In the present study, we employed data from the year 2022. The target population of the survey included 56 213 individuals, of whom 51 850 participated (participation rate, 92.2%). The study population was administered an extensive survey covering various areas including demographics, diet, current physical and mental health, health-related behaviors, and other pertinent factors. The survey questionnaire was composed of 114 questions in total. Out of the 51 850 participants, 1549 were excluded from the study due to incomplete data on demographics (n=86), current physical and mental behavior (n=22), and health-related behavior questionnaires (n=1379). This resulted in a final study population of 50 301 adolescents. Within this group, 2789 individuals reported having engaged in sexual intercourse, forming a subset of participants for the analysis of sexual behavior.
- Unhealthy Adolescent Behaviors
- The variables related to unhealthy behaviors in adolescents included experiences of smoking, alcohol consumption, and unsafe sexual practices. Adolescents who reported consuming alcohol on more than 1 day in the past 30 days were categorized as current drinkers. Similarly, those who reported using any form of tobacco product on more than 1 day in the past 30 days were categorized as current smokers. The variable for unsafe sexual behavior was determined based on contraceptive practices among the sexually active adolescents (n=2789). Participants were divided into 2 groups: those who always or mostly used contraception, indicating safe sexual behavior, and those who occasionally or never used contraception, indicating unsafe sexual behavior.
- Anxiety
- Generalized anxiety disorder (GAD) is a prevalent anxiety disorder characterized by persistent worrying, symptoms of anxiety, and tension in children and adolescents. In this study, anxiety levels were assessed using the Generalized Anxiety Disorder-7 questionnaire (GAD-7). The GAD-7 is a reliable and valid self-report screening tool for generalized anxiety symptoms in adolescents [22]. The GAD-7 consists of 7 questions used to evaluate the individual’s experiences over the prior 2 weeks. Each question is scored on a scale of 0 to 3, with response options reflecting the frequency of the experienced symptom: “not at all,” “several days,” “more than 7 days,” and “nearly every day.” The total GAD-7 score can range from 0 to 21. Based on previous studies, a cut-off point of 10 on the GAD-7 score is interpreted as indicative of anxiety [23,24].
- Physical Activity
- According to both the WHO guidelines on physical activity and the youth physical activity guidelines developed by the Ministry of Health and Welfare in Korea, the criteria for physical activity among youth include participating in more than moderate aerobic physical activity for at least 60 minutes each day and engaging in high-intensity physical activity for a minimum of 3 days per week [9,25]. The number of days in which the criteria were met for more than moderate physical activity, as indicated by an increased heart rate or breathlessness, was evaluated. A separate question was used to assess the number of days that included high-intensity physical activity.
- Other Variables of Interest
- In addition to the primary variables of interest, this study incorporated several demographic and health-related behavior variables, considered other variables of interest. The demographic variables included sex (male or female), school level (middle school or high school), economic status (lower or upper-middle), and cohabitation status regarding parents (none, with 1 parent, or with both parents). Smartphone usage was quantified by the amount of time spent on the device during weekdays. The experience of violence (yes or no) was assessed based on whether medical treatment was sought due to violence-related incidents. Other health-related behavior variables included self-reported sleep quality (good or poor), and daily perceived stress levels (high or low).
- Statistical Analysis
- All statistical analyses were performed using PROC procedures in SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). All tests were 2-sided, with the level of statistical significance established at α=0.05. All variables, except for age and GAD-7 score, were treated as categorical variables.
- To explore the impact of physical activity on the association between anxiety and risk behavior, the participants were divided into exercise and non-exercise groups, based on exercise status as a potential moderating variable. This division was implemented to determine whether the calculated coefficients significantly varied between these groups, thereby validating the presence of interaction effects. In terms of demographics, we utilized an adjusted general linear model to compute the least squares means of the GAD-7 score for each group, based on unhealthy behaviors. Additionally, we conducted an adjusted logistic regression analysis to examine the relationship between the severity of anxiety and physical activity. Odds ratios (ORs) and 95% confidence intervals (CIs) were computed. The models were adjusted for sex, year in school, economic status, cohabitation status, experience of violence, smartphone usage time, sleep quality, perceived stress, and other risk behaviors (current smoking or current alcohol consumption). In these analyses, the independent variables were unhealthy behaviors, while the dependent variables were the presence or absence of anxiety or the GAD-7 score. For the interaction analysis, interaction terms—representing the relationship between individual unhealthy behaviors and physical activity—were included in each model.
- Ethics Statement
- The all data was provided with personal information removed. The ethics approval for this study was waived by the Institutional Review Board under Seoul National University College of Medicine and Seoul National University Hospital (IRB No. E-2307-029-1447).
METHODS
- Participant Characteristics
- Table 1 presents the characteristics of the study population, including the number of participants (n), percentage (%), mean GAD-7 score, standard error (SE), and corresponding p-values for each variable. Of the 50 301 participants, 25 312 were male and 24 989 were female. The mean age of the study population was 15.19 years (SE, 0.01), and the mean GAD-7 score was 4.23 (SE, 0.02). Higher mean GAD-7 scores were significantly associated with male sex (p<0.001), older age (p<0.001), high school student status (p<0.001), lower economic class (p<0.001), living with a single parent (p<0.001), and having experienced violence (p<0.001). Additional factors contributing to higher mean GAD-7 scores included poor sleep (p<0.001), higher perceived stress (p<0.001), current smoking (p<0.001), current alcohol consumption (p<0.001), a lack of regular exercise (p<0.001), and having engaged in sexual intercourse (p<0.001), particularly when unsafe sexual behavior was involved (p<0.001).
- Distribution of Anxiety
- Table 2 displays the distribution of anxiety levels (ranging from none to severe) among the participants, categorized by their engagement in unhealthy behaviors. Significantly higher levels of anxiety were observed among smokers compared to non-smokers (p<0.001) and among drinkers compared to nondrinkers (p<0.001). Furthermore, a significant difference in anxiety levels was also noted between participants who practiced safe sexual behaviors and those who did not (p=0.032). These findings suggest that individuals who engage in smoking, alcohol consumption, or unsafe sexual behaviors tend to experience a greater degree of anxiety.
- Table 3 presents the number of participants with or without anxiety, categorized by their engagement in unhealthy behavior. Of 50 301 participants, 3109 individuals adhered to the guidelines for physical activity, constituting the exercise group, while the remaining 47 192 participants did not engage in regular physical activity, forming the non-exercise group. Within the exercise group, the prevalence of anxiety was significantly lower in non-smokers and non-drinkers compared to smokers (p=0.006) and drinkers (p<0.001). However, no statistically significant difference in the prevalence of anxiety was observed between individuals who engaged in unsafe sexual behaviors and those who did not (p=0.319). In the non-exercise group, non-smokers, non-drinkers, and those not engaging in unsafe sexual behavior also had a significantly lower prevalence of anxiety compared to smokers (p<0.001), drinkers (p<0.001), and those who engaged in such behavior (p=0.029). Upon introducing interaction terms between risky behaviors (smoking, alcohol consumption, and unsafe sexual behavior) and exercise, none of these interaction terms were found to be statistically significant (p=0.373, 0.208, and 0.734, respectively).
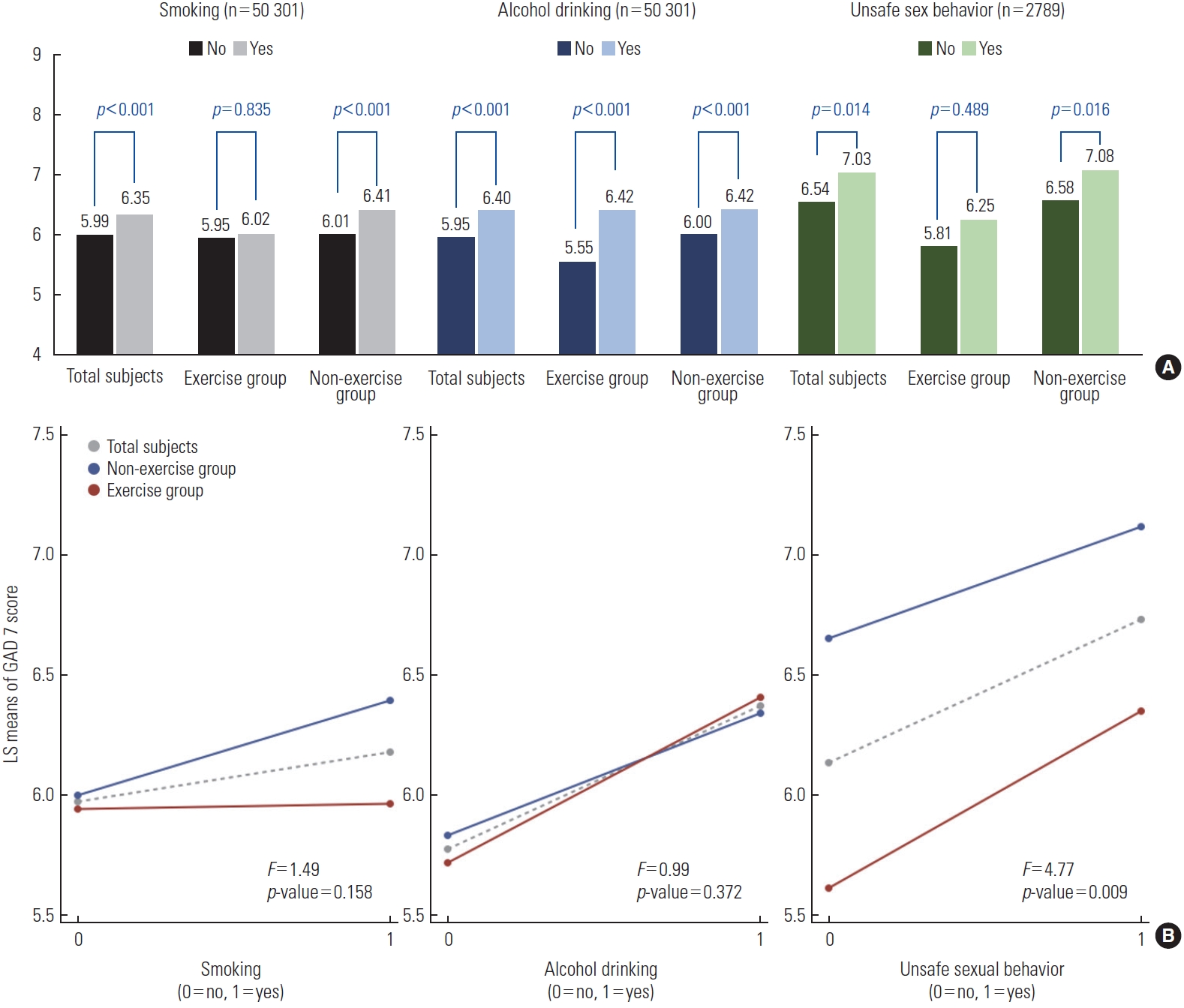
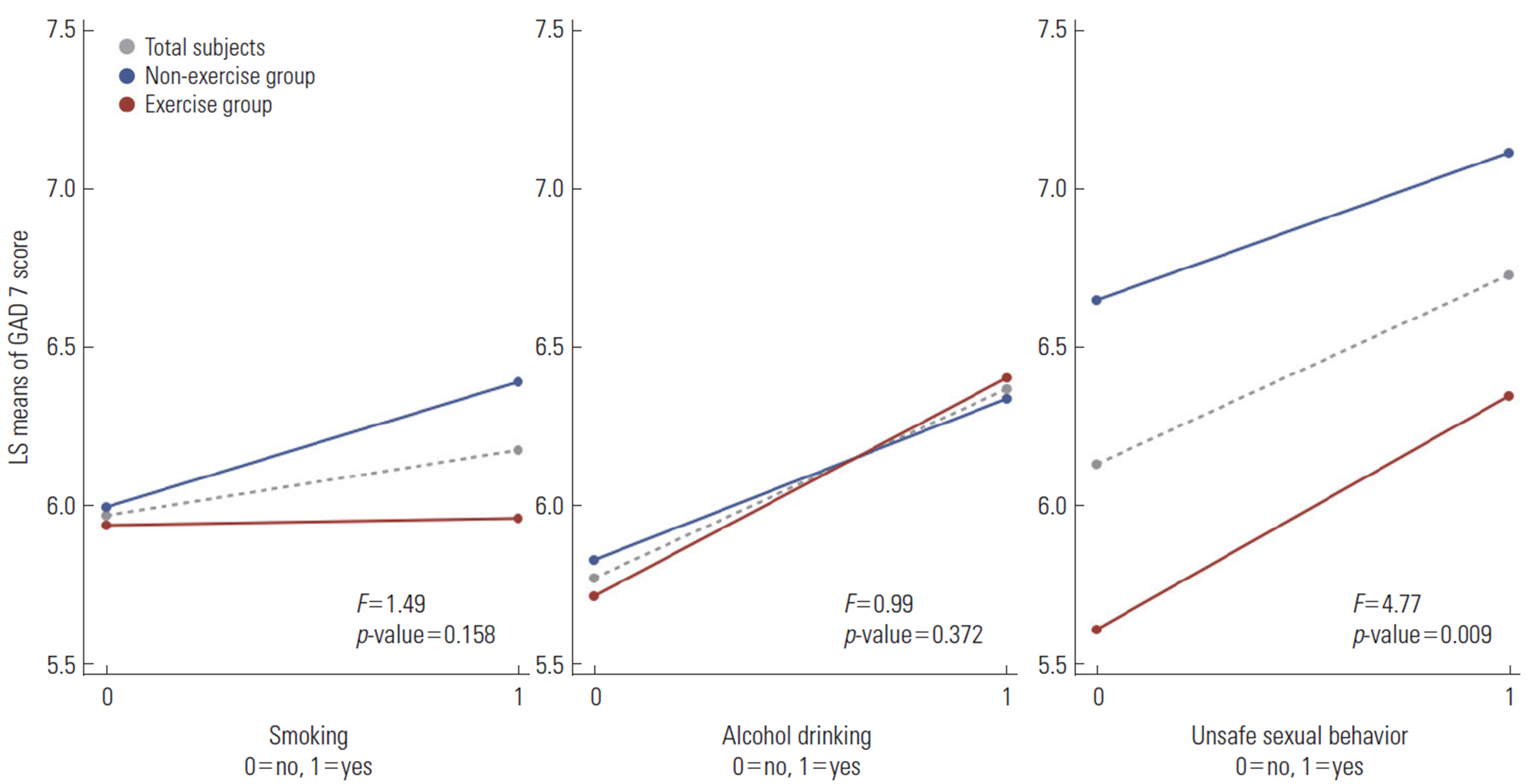
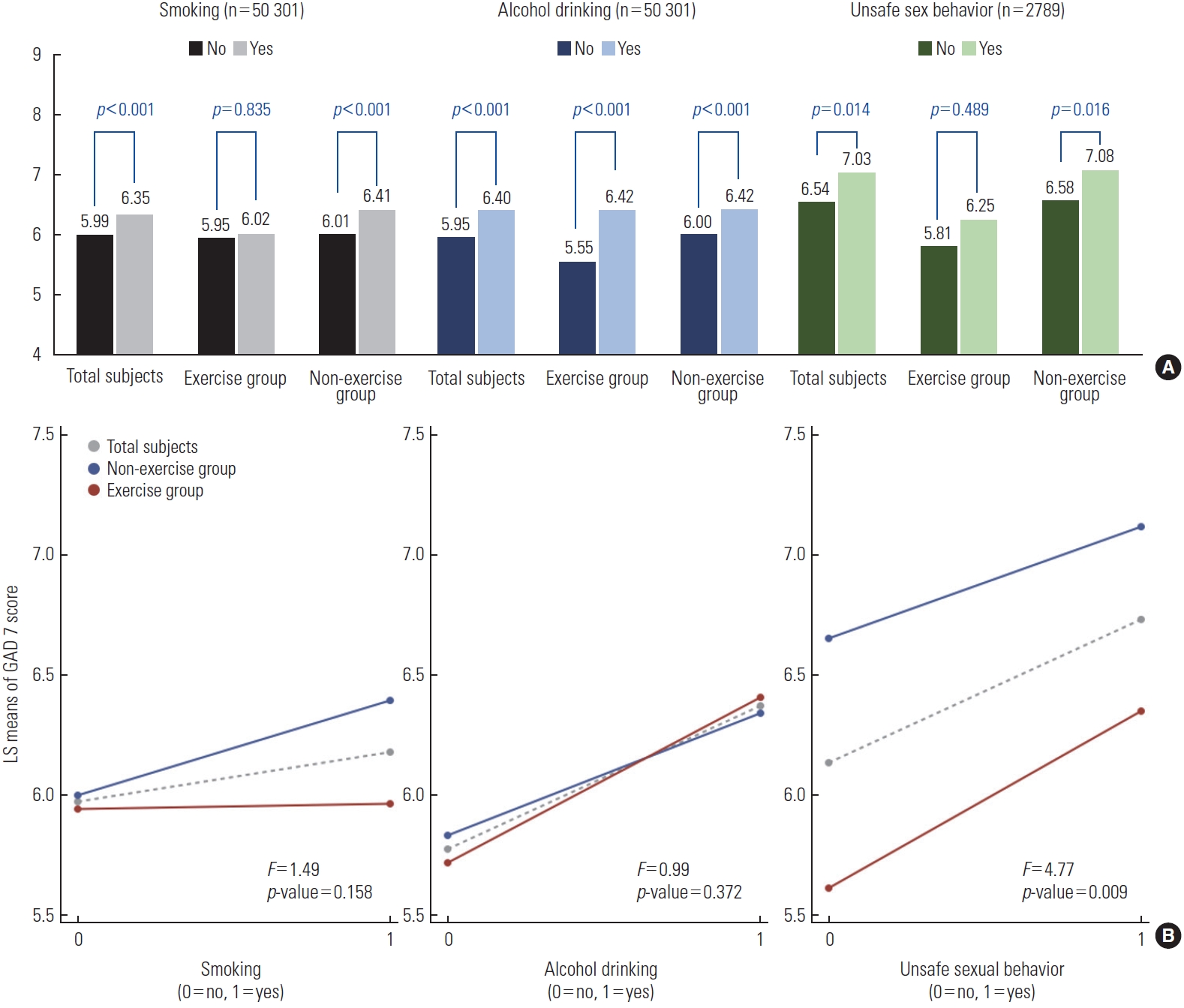
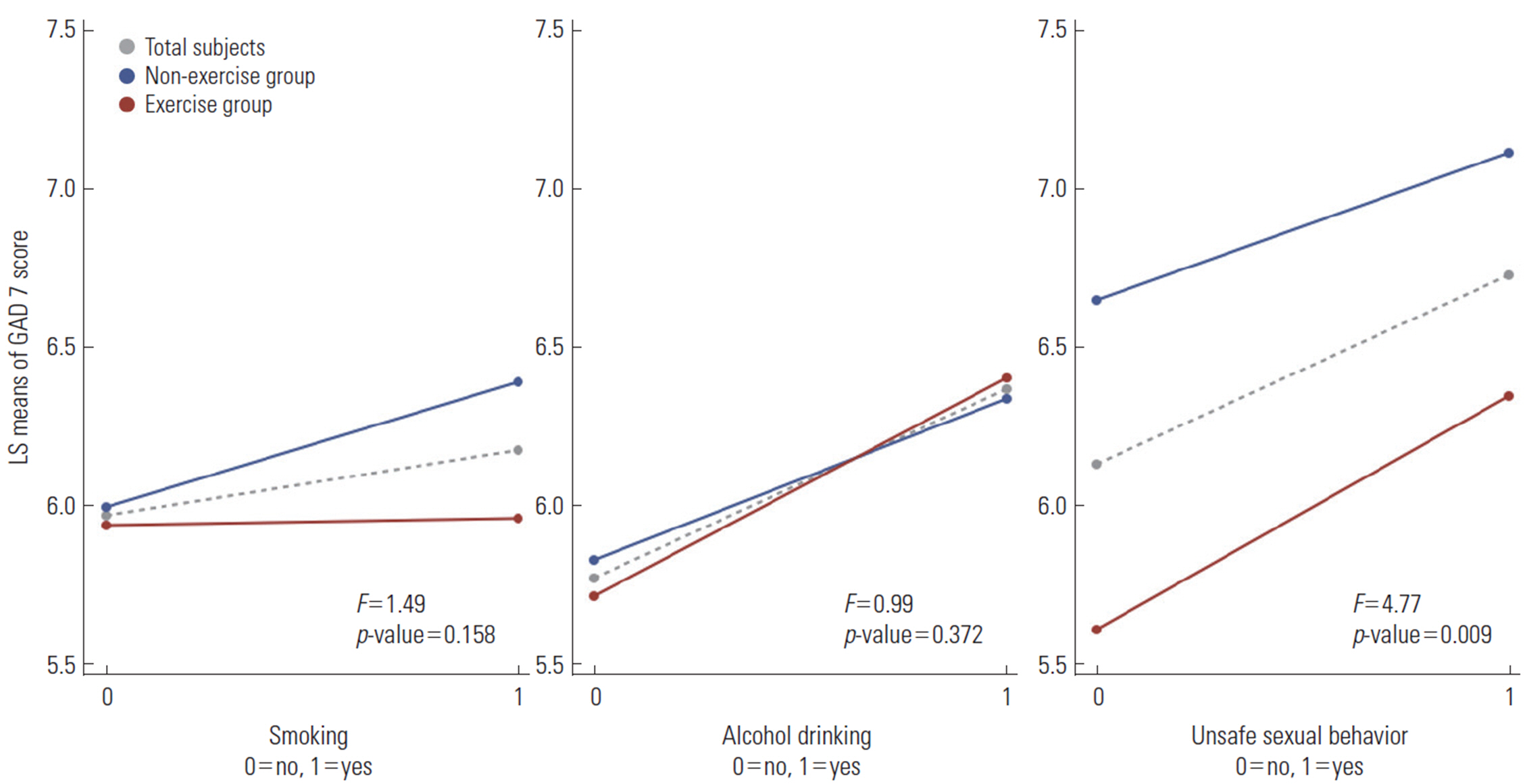
- Anxiety Scores by Unhealthy Behavior and Physical Activity
- Figure 1 shows the least squares means of participants’ GAD-7 scores, categorized by unhealthy behaviors and physical activity. Across all participants, current smokers exhibited a higher mean GAD-7 score than non-smokers (6.35 vs. 5.99, respectively; p<0.001). Similarly, current drinkers displayed a higher mean GAD-7 score than non-drinkers (6.40 vs. 5.95, respectively; p<0.001). Adolescents who engaged in unsafe sexual behaviors had a mean GAD-7 score of 7.03, whereas those who practiced safe sexual behaviors had a lower mean score, at 6.54 (p=0.014). Upon stratification by physical activity engagement, the non-exercise group exhibited significant differences in GAD-7 scores in relation to current smoking, current alcohol consumption, and unsafe sexual behaviors (p<0.001, <0.001, and 0.016, respectively). However, within the exercise group, the differences in GAD-7 scores for current smoking or unsafe sexual behavior were not significant (p=0.835 and 0.489, respectively). The interaction effects between smoking and exercise, and between drinking and exercise, were not significant in the analysis (p=0.158 and 0.372, respectively). However, the interaction effect between unsafe sexual behavior and exercise was significant (F=4.77, p=0.009).
- Anxiety by Unhealthy Behavior and Physical Activity
- Table 4 presents the results of a logistic regression analysis examining the relationship between anxiety and unhealthy behaviors in adolescents, segmented by physical activity. The reference group was defined as including participants who did not engage in each unhealthy behavior. Across all participants, the adjusted model revealed a significant positive relationship between current smoking and anxiety (OR, 1.34; 95% CI, 1.16 to 1.54). Similarly, significant positive relationships were found between unsafe sexual behavior and anxiety (OR, 1.33; 95% CI, 1.04 to 1.71). Within the non-exercise group, the positive relationships remained significant, both between anxiety and current smoking (OR, 1.36; 95% CI, 1.18 to 1.57) and between anxiety and unsafe sex (OR, 1.33; 95% CI, 1.02 to 1.73). However, among participants who exercised, no significant associations were found between anxiety and current smoking, or between anxiety and unsafe sexual behavior. Regarding alcohol consumption, significant positive relationships were found between current drinking and anxiety, irrespective of exercise status. However, the interaction effects between each unhealthy behavior and exercise were not significant (smoking, p=0.373; alcohol consumption, p=0.208; unsafe sexual behavior, p=0.734).
RESULTS
- Summary
- In this study, we examined the impact of exercise on the relationship between unhealthy behaviors during adolescence and anxiety among students in Korea. We found that individuals who engaged in smoking, alcohol consumption, or unsafe sexual behavior tended to experience more severe anxiety. When we stratified the data based on physical activity, we found no significant differences in GAD-7 score within the exercise group between current smokers and non-smokers, or between those who did and did not engage in unsafe sexual behavior. However, within the non-exercise group, anxiety scores were significantly lower among those who did not engage in unhealthy behaviors than those who did, with the exception of alcohol consumption. In the regression model, only the interaction between unsafe sex behavior and exercise was significant, while the other interaction terms with smoking or alcohol were not. In the logistic regression analysis, within the non-exercise group, anxiety was significantly positively associated with both smoking and unsafe sexual behavior. However, this relationship was not evident within the exercise group. Alcohol consumption did not demonstrate a similar trend in relation to anxiety within either the exercise or non-exercise groups. In terms of interaction, none of the interactions between unhealthy behaviors and exercise were significant in the adjusted logistic regression model.
- Adolescent Unhealthy Behaviors and Anxiety
- Numerous studies have substantiated the reciprocal relationships between unhealthy behaviors in adolescents and anxiety disorders. Adolescents who currently smoke or drink are susceptible to anxiety, and those with anxiety are inclined to smoke and consume alcohol. A longitudinal investigation revealed that smoking more than 20 cigarettes per day during adolescence was associated with GAD in early adulthood (OR, 5.53; 95% CI, 1.84 to 16.66) [26]. The quantity and frequency of cigarette smoking were also associated with GAD (OR, 1.36; 95% CI, 1.07 to 1.71). This result could be explained by the potential roles of neurotransmitter systems, inflammation, oxidative and nitrosative stress, mitochondrial dysfunction, and epigenetic effects in the pathogenesis of anxiety [15]. Psychological factors have also been linked to unsafe sexual behavior among adolescents. According to a study in Slovakia, students in early adolescence who exhibited anxiety or depression were particularly likely to engage in unsafe sex (OR, 1.07; 95% CI, 1.02 to 1.12) [27].
- Regarding alcohol use, heavy drinking early in adolescence has been shown to be associated with an increased risk of anxiety due to heightened vulnerability in the developing brain [13]. In a cross-sectional study of Norwegian secondary school students [28], more severe anxiety symptoms were associated with alcohol use among girls. However, a 2019 longitudinal study in Pittsburgh did not consistently find an association between the severity of anxiety and alcohol use [29]. In the present study, the pattern observed among alcohol drinkers did not align with that of smokers or individuals who engaged in unsafe sexual behavior. This discrepancy may be due to a strong reciprocal relationship between alcohol consumption and anxiety, a relationship that cannot be overcome simply with regular exercise. Moreover, the odds ratio for anxiety and alcohol use was higher in the exercise group than in the non-exercise group, a finding that calls for further research.
- Exercise
- It has been relatively well established that physical exercise can reduce anxiety in both adults and adolescents [18,19,30]. In the general population, an inverse correlation has frequently been observed between physical activity and the incidence or symptoms of anxiety disorders [31]. A large populationbased study in the Netherlands revealed that individuals who exercised were, on average, less anxious (standard difference, -0.18) than non-exercisers, provided they exercised for at least 60 minutes per week with a metabolic equivalent of task score of 4 or higher [32]. A 6-month randomized exercise intervention applied among Swedish girls also revealed that the group who exercised displayed significant differences in Social Physique Anxiety Scale scores compared to non-exercisers (p<0.05). Although most randomized controlled trials have suggested benefits of exercise for reducing anxiety, methodological limitations remain [33].
- The absence of the relationship in the exercise group in this study could be attributed to the same pathology by which exercise mitigates anxiety. Although the exact mechanism behind exercise’s prevention of anxiety is not fully understood, several potential mechanisms have been suggested [28]. Regular aerobic exercise is associated with reduced activity in the sympathetic nervous system and the hypothalamic-pituitary-adrenal axis. Furthermore, exercise influences the release of corticotrophin-releasing factor and adrenocorticotropic hormone [34]. From a physiological perspective, enhancing self-efficacy through managing the stress of exercise and diverting attention away from stressors may also contribute to decreased anxiety in adolescents [28,35]. This is particularly relevant as adolescent smoking and sexual behaviors have been specifically associated with lower self-efficacy or self-esteem [36].
- However, this information does not necessarily suggest that exercise yields positive effects on unhealthy behaviors. For instance, among 8 randomized controlled trials on smoking, only 2 identified a positive effect of exercise on abstinence from smoking [37]. Furthermore, another meta-analysis concluded that exercise did not result in decreased alcohol consumption, while it was not feasible to investigate the moderating effects of smoking [38].
- Likewise, based on the findings of the present study, physical activity cannot be said to significantly influence the relationship between unhealthy behaviors and anxiety. The interaction term did not yield statistically significant results, indicating that exercise does not function as an interacting or moderating variable in this relationship. However, it is still possible that exercise may affect the relationship between unhealthy behaviors and anxiety in other ways or from different perspectives. This is because the estimated coefficients varied significantly between groups when verifying the interaction effect in the divided samples.
- Strengths and Limitations
- To our knowledge, this is the first study to evaluate the impact of physical activity on the relationship between unhealthy behaviors in adolescents and anxiety, utilizing a large student dataset. Nonetheless, this study had limitations. First, due to its cross-sectional design, causality could not be definitively established. Additionally, a confounding effect may have been present. We employed an adjusted model with multiple covariates, but we cannot rule out the possibility of a residual confounding effect from unmeasured or external factors, such as the consumption of coffee or other substances potentially increasing anxiety in adolescents. Moreover, the data for smoking, alcohol use, unsafe sexual behavior, GAD-7 score, and exercise were self-reported, which could have led to inaccuracies or bias, particularly given the public-school setting of the survey. The results may vary depending on the definitions or measurement methods used for exercise and such behaviors. Additionally, variations in sample size across variables could have impacted the CIs and significance levels of these analyses. For instance, the limited number of individuals engaging in unsafe sexual behavior may have influenced the results. The effect size can also impact statistical outcomes; that is, if the actual size of the interaction effect between unhealthy behavior and exercise was small, detection would be difficult. Due to data limitations, we were unable to directly estimate the inherent interaction effects when examining differences between groups with regard to interaction effects [39].
- In this study, we were unable to find evidence suggesting that exercise influences the relationship between adolescent unhealthy behaviors and anxiety. Contrary to popular belief, our findings indicate that physical activity may not serve as a cost-effective intervention for adolescent anxiety arising from unhealthy behaviors. We recommend further research, considering the potential for minor interaction effects, measurement methods, external factors, and the presence or absence of other confounding variables.
DISCUSSION
-
CONFLICT OF INTEREST
The authors have no conflicts of interest associated with the material presented in this paper.
-
FUNDING
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF), funded by the Ministry of Education, Science and Technology (grant number, 2022R1A2C2010463).
-
AUTHOR CONTRIBUTIONS
Conceptualization: Lee HJ, Min KB. Data curation: Lee HJ, Choi JP, Oh K. Formal analysis: Lee HJ. Funding acquisition: Min JY, Min KB. Methodology: Lee HJ, Min JY, Min KB. Writing – original draft: Lee HJ, Choi JP, Oh K. Writing – review & editing: Lee HJ, Min JY, Min KB.
Notes
ACKNOWLEDGEMENTS
| Variables | Total participants | p-value | Interaction term (p-value)1 | Exercise group | p-value | Non-exercise group | p-value | ||
|---|---|---|---|---|---|---|---|---|---|
| Current smoking | <0.001 | 0.403 | 0.006 | <0.001 | |||||
| Subject (n) | 50 301 | 3109 | 47 192 | ||||||
| No | |||||||||
| No anxiety | 41 956 (87.6) | 2551 (87.9) | 39 405 (87.6) | ||||||
| Anxiety | 5894 (12.3) | 349 (12.0) | 5545 (12.3) | ||||||
| Yes | |||||||||
| No anxiety | 1950 (79.5) | 172 (82.2) | 1778 (79.3) | ||||||
| Anxiety | 501 (20.4) | 37 (17.7) | 464 (20.6) | ||||||
| Current alcohol use | <0.001 | 0.126 | <0.001 | <0.001 | |||||
| Subject (n) | 50 301 | 3109 | 47 192 | ||||||
| No | |||||||||
| No anxiety | 38 634 (87.9) | 2324 (88.8) | 36 310 (87.9) | ||||||
| Anxiety | 5281 (12.0) | 292 (11.1) | 4989 (12.0) | ||||||
| Yes | |||||||||
| No anxiety | 5272 (82.5) | 399 (80.9) | 4873 (82.6) | ||||||
| Anxiety | 1114 (17.4) | 94 (19.0) | 1020 (17.3) | ||||||
| Unsafe sexual behavior | 0.019 | 0.331 | 0.319 | 0.029 | |||||
| Subject (n) | 2789 | 266 | 2523 | ||||||
| No | |||||||||
| No anxiety | 1502 (82.2) | 143 (87.1) | 1359 (81.7) | ||||||
| Anxiety | 325 (17.7) | 21 (12.8) | 304 (18.2) | ||||||
| Yes | |||||||||
| No anxiety | 753 (78.2) | 81 (79.4) | 672 (78.1) | ||||||
| Anxiety | 209 (21.7) | 21 (20.5) | 188 (21.8) | ||||||
| Variables | Total participants | Interaction term (p-value)2 | Exercise group | Non-exercise group |
|---|---|---|---|---|
| Current smoking | ||||
| Subject (n) | 50 301 | 3109 | 47 192 | |
| No | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |
| Yes | 1.34 (1.16, 1.54)* | 0.373 | 1.18 (0.70, 2.00) | 1.36 (1.18, 1.57)* |
| Current alcohol use | ||||
| Subject (n) | 50 301 | 3109 | 47 192 | |
| No | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |
| Yes | 1.18 (1.08, 1.3)* | 0.208 | 1.96 (1.37, 2.81)* | 1.14 (1.03, 1.26)* |
| Unsafe sexual behavior | ||||
| Subject (n) | 2789 | 266 | 2523 | |
| No | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |
| Yes | 1.33 (1.04, 1.71)* | 0.734 | 1.38 (0.58, 3.32) | 1.33 (1.02, 1.73)* |
Values are presented as odds ratio (95% confidence interval).
1 The regression model was adjusted for sex, year in school, economic status, cohabitation status, experience of violence, smartphone usage, sleep quality, perceived stress, and other risk behaviors (current smoking or current alcohol use).
2 Interaction between each unhealthy behavior and exercise (that is, smoking and exercise, alcohol drinking and exercise, and unsafe sexual behavior and exercise).
* p<0.05.
- 1. Buchmann AF, Schmid B, Blomeyer D, Becker K, Treutlein J, Zimmermann US, et al. Impact of age at first drink on vulnerability to alcohol-related problems: testing the marker hypothesis in a prospective study of young adults. J Psychiatr Res 2009;43(15):1205-1212ArticlePubMed
- 2. Esser MB, Guy GP Jr, Zhang K, Brewer RD. Binge drinking and prescription opioid misuse in the U.S., 2012-2014. Am J Prev Med 2019;57(2):197-208ArticlePubMedPMC
- 3. Miller JW, Naimi TS, Brewer RD, Jones SE. Binge drinking and associated health risk behaviors among high school students. Pediatrics 2007;119(1):76-85ArticlePubMedPDF
- 4. Ju YJ, Kim W, Oh SS, Park EC. Solitary drinking and the risk of depressive symptoms and suicidal ideation in college students: findings from a nationwide survey in Korea. J Affect Disord 2019;257: 710-715ArticlePubMed
- 5. Park SH. Smoking and adolescent health. Korean J Pediatr 2011;54(10):401-404ArticlePubMedPMC
- 6. Wang TW, Gentzke A, Sharapova S, Cullen KA, Ambrose BK, Jamal A. Tobacco product use among middle and high school students - United States, 2011-2017. MMWR Morb Mortal Wkly Rep 2018;67(22):629-633ArticlePubMedPMC
- 7. Ho SY, Chen J, Leung LT, Mok HY, Wang L, Wang MP, et al. Adolescent smoking in Hong Kong: prevalence, psychosocial correlates, and prevention. J Adolesc Health 2019;64(6S):S19-S27ArticlePubMed
- 8. Hoots BE, Li J, Hertz MF, Esser MB, Rico A, Zavala EY, et al. Alcohol and other substance use before and during the COVID-19 pandemic among high school students - Youth Risk Behavior Survey, United States, 2021. MMWR Suppl 2023;72(1):84-92ArticlePubMedPMC
- 9. Ministry of Health and Welfare. The physical activity guidelines for Koreans. 2013 [cited 2023 Apr 1]. Available from: https://www.mohw.go.kr/board.es?mid=a10411010300&bid=0019&act=view&list_no=337139 (Korean)
- 10. Maeng SJ, Lee DJ, Kang JH. First drinking experiences during adolescence in South Korea: a qualitative study focusing on the internal and external factors. Int J Environ Res Public Health 2021;18(15):8200ArticlePubMedPMC
- 11. Kassa BG, Belay HG, Ayele AD. Teenage pregnancy and its associated factors among teenage females in Farta Woreda, Northwest, Ethiopia, 2020: a community-based cross-sectional study. Popul Med 2021;3(July):19ArticlePDF
- 12. McKenzie M, Jorm AF, Romaniuk H, Olsson CA, Patton GC. Association of adolescent symptoms of depression and anxiety with alcohol use disorders in young adulthood: findings from the Victorian Adolescent Health Cohort Study. Med J Aust 2011;195(3):S27-S30ArticlePubMedPDF
- 13. Gilpin NW, Karanikas CA, Richardson HN. Adolescent binge drinking leads to changes in alcohol drinking, anxiety, and amygdalar corticotropin releasing factor cells in adulthood in male rats. PLoS One 2012;7(2):e31466ArticlePubMedPMC
- 14. Rosenthal D, Moore S, Flynn I. Adolescent self‐efficacy, self‐esteem and sexual risk‐taking. J Community Appl Soc Psychol 1991;1(2):77-88Article
- 15. Moylan S, Jacka FN, Pasco JA, Berk M. How cigarette smoking may increase the risk of anxiety symptoms and anxiety disorders: a critical review of biological pathways. Brain Behav 2013;3(3):302-326ArticlePubMedPMC
- 16. Kushner MG, Abrams K, Borchardt C. The relationship between anxiety disorders and alcohol use disorders: a review of major perspectives and findings. Clin Psychol Rev 2000;20(2):149-171ArticlePubMed
- 17. Silberman Y, Bajo M, Chappell AM, Christian DT, Cruz M, Diaz MR, et al. Neurobiological mechanisms contributing to alcohol-stress-anxiety interactions. Alcohol 2009;43(7):509-519ArticlePubMedPMC
- 18. Paluska SA, Schwenk TL. Physical activity and mental health: current concepts. Sports Med 2000;29(3):167-180PubMed
- 19. Carek PJ, Laibstain SE, Carek SM. Exercise for the treatment of depression and anxiety. Int J Psychiatry Med 2011;41(1):15-28ArticlePubMedPDF
- 20. Marquez DX, Jerome GJ, McAuley E, Snook EM, Canaklisova S. Self-efficacy manipulation and state anxiety responses to exercise in low active women. Psychol Health 2002;17(6):783-791Article
- 21. Kim Y, Choi S, Chun C, Park S, Khang YH, Oh K. Data resource profile: the Korea Youth Risk Behavior Web-based Survey (KYRBS). Int J Epidemiol 2016;45(4):1076-1076eArticlePubMed
- 22. Tiirikainen K, Haravuori H, Ranta K, Kaltiala-Heino R, Marttunen M. Psychometric properties of the 7-item Generalized Anxiety Disorder Scale (GAD-7) in a large representative sample of Finnish adolescents. Psychiatry Res 2019;272: 30-35ArticlePubMed
- 23. Mossman SA, Luft MJ, Schroeder HK, Varney ST, Fleck DE, Barzman DH, et al. The Generalized Anxiety Disorder 7-item scale in adolescents with generalized anxiety disorder: signal detection and validation. Ann Clin Psychiatry 2017;29(4):227-234APubMedPMC
- 24. Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med 2006;166(10):1092-1097ArticlePubMed
- 25. World Health Organization. WHO guidelines on physical activity and sedentary behavior. 2020 [cited 2023 Jul 1]. Available from: https://www.who.int/publications/i/item/9789240015128
- 26. Johnson JG, Cohen P, Pine DS, Klein DF, Kasen S, Brook JS. Association between cigarette smoking and anxiety disorders during adolescence and early adulthood. JAMA 2000;284(18):2348-2351ArticlePubMed
- 27. Kalina O, Geckova AM, Klein D, Jarcuska P, Orosova O, van Dijk JP, et al. Psychosocial factors associated with sexual behaviour in early adolescence. Eur J Contracept Reprod Health Care 2011;16(4):298-306ArticlePubMed
- 28. Anderson E, Shivakumar G. Effects of exercise and physical activity on anxiety. Front Psychiatry 2013;4: 27ArticlePubMedPMC
- 29. Schleider JL, Ye F, Wang F, Hipwell AE, Chung T, Sartor CE. Longitudinal reciprocal associations between anxiety, depression, and alcohol use in adolescent girls. Alcohol Clin Exp Res 2019;43(1):98-107ArticlePubMedPMCPDF
- 30. Scully D, Kremer J, Meade MM, Graham R, Dudgeon K. Physical exercise and psychological well being: a critical review. Br J Sports Med 1998;32(2):111-120ArticlePubMedPMC
- 31. Teychenne M, Costigan SA, Parker K. The association between sedentary behaviour and risk of anxiety: a systematic review. BMC Public Health 2015;15: 513ArticlePubMedPMCPDF
- 32. De Moor MH, Beem AL, Stubbe JH, Boomsma DI, De Geus EJ. Regular exercise, anxiety, depression and personality: a population-based study. Prev Med 2006;42(4):273-279ArticlePubMed
- 33. Stonerock GL, Hoffman BM, Smith PJ, Blumenthal JA. Exercise as treatment for anxiety: systematic review and analysis. Ann Behav Med 2015;49(4):542-556ArticlePubMedPMC
- 34. Droste SK, Gesing A, Ulbricht S, Müller MB, Linthorst AC, Reul JM. Effects of long-term voluntary exercise on the mouse hypothalamic-pituitary-adrenocortical axis. Endocrinology 2003;144(7):3012-3023ArticlePubMed
- 35. Sonstroem RJ. Physical activity and self-esteem. In: Morgan WP, editor. Physical activity and mental health. London: Taylor & Francis; 2013. p. 127-143
- 36. Ayar D, Bektas M, Bektas I, Sal Altan S, Ayar U. Effects of adolescents’ self-efficacy and social anxiety on attitudes toward pros and cons of smoking. J Subst Use 2019;24(1):8-14Article
- 37. Ussher MH, Taylor AH, West R, McEwen A. Does exercise aid smoking cessation? A systematic review. Addiction 2000;95(2):199-208ArticlePubMedPDF
- 38. Hallgren M, Vancampfort D, Giesen ES, Lundin A, Stubbs B. Exercise as treatment for alcohol use disorders: systematic review and meta-analysis. Br J Sports Med 2017;51(14):1058-1064ArticlePubMed
- 39. Hong SH, Jung S. Testing the interaction effects in regression and structural equation models: theories and procedures. Korean J Hum Dev 2014;21(4):1-24. (Korean)Article
REFERENCES
Figure & Data
References
Citations
 PubReader
PubReader ePub Link
ePub Link Cite
Cite- Figure
-
- Related articles
-
- Association Between Objective Social Isolation and Unmet Medical Needs: A Nationwide Cross-sectional Study in Korea
- The Effect of Cognitive Impairment on the Association Between Social Network Properties and Mortality Among Older Korean Adults
- Open Communication About Reproductive Health Is Associated With Comprehensive HIV Knowledge and a Non-stigmatising Attitude Among Indonesian Youth: A Cross-sectional Study
- Association Between Sleep Quality and Anxiety in Korean Adolescents

