Articles
- Page Path
- HOME > J Prev Med Public Health > Volume 52(6); 2019 > Article
-
Original Article
Sex-specific Associations Between Serum Hemoglobin Levels and the Risk of Cause-specific Death in Korea Using the National Health Insurance Service-National Health Screening Cohort (NHIS HEALS) -
Yoonsuk An1,2
 , Jieun Jang1,2,3, Sangjun Lee1,2,3, Sungji Moon1,2, Sue K. Park1,2,3,4
, Jieun Jang1,2,3, Sangjun Lee1,2,3, Sungji Moon1,2, Sue K. Park1,2,3,4 -
Journal of Preventive Medicine and Public Health 2019;52(6):393-404.
DOI: https://doi.org/10.3961/jpmph.19.146
Published online: November 1, 2019
1Department of Preventive Medicine, Seoul National University College of Medicine, Seoul, Korea
2Cancer Research Institute, Seoul National University, Seoul, Korea
3Department of Biomedical Science, Seoul National University Graduate School, Seoul, Korea
4Interdisciplinary Program in Cancer Biology, Seoul National University College of Medicine, Seoul, Korea
- Corresponding author: Sue K. Park, MD, PhD Department of Preventive Medicine, Seoul National University College of Medicine, 103 Daehak-ro, Jongno-gu, Seoul 03080, Korea E-mail: suepark@snu.ac.kr
Copyright © 2019 The Korean Society for Preventive Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Objectives
- The purpose of this study was to determine the associations between blood hemoglobin (Hgb) levels and the risk of death by specific causes.
-
Methods
- Using the National Health Insurance Services-National Health Screening Cohort (n=487 643), we classified serum Hgb levels into 6 sex-specific groups. Cox regression analysis was used to analyze the associations between Hgb levels and the risk of cause-specific death.
-
Results
- Hgb levels in male population showed a U-shaped, J-shaped, or inverse J-shaped association with the risk of death from ischemic heart disease, acute myocardial infarction, liver cancer, cirrhosis and chronic obstructive pulmonary disease (COPD) (all non-linear p<0.05; hazard ratio [HR]; 95% confidence interval [CI]) for the lowest and the highest Hgb levels for the risk of each cause of death in male population: HR, 1.14; 95% CI, 0.98 to 1.34; HR, 2.87; 95% CI, 1.48 to 5.57; HR, 1.16; 95% CI, 0.96 to 1.40; HR, 3.05; 95% CI, 1.44 to 6.48; HR, 1.36; 95% CI, 1.18 to 1.56; HR, 2.11; 95% CI, 1.05 to 4.26; HR, 3.64; 95% CI, 2.49 to 5.33; HR, 5.97; 95% CI, 1.44 to 24.82; HR, 1.62; 95% CI, 1.14 to 2.30; HR, 3.84; 95% CI, 1.22 to 12.13, respectively), while in female population, high Hgb levels were associated with a lower risk of death from hypertension and a higher risk of death from COPD (overall p<0.05; HR, 1.86; 95% CI, 1.29 to 2.67 for the lowest Hgb levels for hypertension; overall p<0.01, HR, 6.60; 95% CI, 2.37 to 18.14 for the highest Hgb levels for COPD). For the risk of lung cancer death by Hgb levels, a linear negative association was found in male population (overall p<0.01; the lowest Hgb levels, HR, 1.17; 95% CI, 1.05 to 1.33) but an inverse J-shaped association was found in female population (non-linear p=0.01; HR, 1.25; 95% CI, 0.96 to 1.63; HR, 2.58; 95% CI, 1.21 to 5.50).
-
Conclusions
- Both low and high Hgb levels were associated with an increased risk of death from various causes, and some diseases showed different patterns according to sex.
- Blood hemoglobin (Hgb) levels are a non-specific marker for which abnormal findings are found in chronic diseases such as cardiovascular disease (CVD), malignant tumors, and hematological diseases [1,2]. Previous studies have emphasized that low serum Hgb levels increase the risk of death from various diseases, including CVD and cancer [3-5]. However, very few studies have evaluated the effects of high Hgb levels on various types of cause-specific mortality.
- Additionally, the extent to which Hgb levels affect cause-specific mortality differs according to sex. Sex differences in the associations between Hgb levels and the outcomes of CVDs, such as stroke, have been evaluated in a few studies [6-8]. Differences in mortality according to sex might be caused by physiological factors such as menopause, lean body mass, or puberty, which are known to be relevant both for individuals and at the population level [9]. To our best knowledge, although some suggestions have been made regarding possible sex differences in the associations between Hgb levels and patterns of mortality, no studies have evaluated the effect of sex on associations between Hgb levels and mortality from various causes. In order to assess these effects, we conducted an analysis of a large population cohort that contains a relatively large number of instances of cause-specific mortality.
- In this study, we hypothesized that the risk of death from some diseases would be affected by low Hgb levels, while the risk of death from other diseases might also be affected by high Hgb levels. Additionally, we hypothesized that these associations between Hgb levels and death would differ according to sex. Therefore, in this study, we evaluated sex-specific associations of both low and high sex-specific Hgb levels with the risk for death from various diseases, including all causes, CVD, and malignancy, stratified by sex.
INTRODUCTION
- Data Collection and Selection of Study Population
- We used the National Health Insurance Service-National Health Screening Cohort (NHIS-HEALS) database, which consists of 514 795 participants who were enrolled in a health screening program provided by the NHIS in Korea. Baseline recruitment was performed in 2002 and 2003; the participants were between 40 years and 79 years of age, and were followed until 2013 [10]. Anthropometric variables (e.g., height and weight), laboratory blood and urine tests (e.g., serum Hgb levels, alanine aminotransferase levels, and aspartate aminotransferase levels), and information based on self-reported questionnaires were gathered in the baseline year. Blood tests, including Hgb levels, were conducted using samples collected at health check-ups at different healthcare centers. We excluded participants who died within 2 years from baseline (n=4522) because we thought that it would take more than 2 years for baseline serum Hgb levels to affect participants’ likelihood of death. Subjects with missing information on serum Hgb levels were excluded (n=584). We further excluded participants with a past history of diseases of blood and blood-forming organs (n=13 429). Additionally, we excluded participants with diseases that are known to possibly affect Hgb levels such as hematopoietic neoplasms (n=44), autoimmune diseases such as rheumatoid arthritis and systematic lupus erythematosus (n=7085), inflammatory bowel diseases such as ulcerative colitis and Crohn’s disease (n=1065) and chronic kidney diseases (n=423). We used International Statistical Classification of Diseases and Related Health Problems (ICD)-10 codes to identify the above diseases. In total, we analyzed 487 643 subjects [11]. A schematic illustration of the selection of the study population is presented in Supplemental Material 1.
- Outcome Variables
- The outcome variables in this study were all-cause death and deaths caused by specific diseases. Deaths were classified according to ICD-10 codes as follows: (1) all-cause deaths were defined by the ICD-10 codes A00-Z99; (2) CVD deaths were defined by the ICD-10 codes I00-I99, and subdivided into those caused by ischemic heart disease (IHD; I20-I25), acute myocardial infarction (AMI; I21), hypertension (I10-I16), total stroke (I60-I69), hemorrhagic stroke (I60-I62), and ischemic stroke (I63); and (3) total cancer deaths were defined by the ICD-10 codes C00-C97, and subdivided into lung cancer (C34), gastric cancer (C16), colon cancer (C18-C20), and liver cancer (C22). Other diseases, including chronic obstructive pulmonary disease (COPD; J44), and liver cirrhosis including fibrosis (K74) were defined by the respective ICD-10 code. The follow-up period of participants extended from the date of enrollment to the date of death or to December 31, 2013.
- Exposure Variables
- A total of 487 643 participants underwent blood and urine tests. Our exposure variable was serum Hgb, and we set the lowest range of concentrations (g/dL) as Hgb<14.0 for males and Hgb<12.0 for females. Next, we further separated our participants by Hgb levels of 1 g/dL, resulting in the following classification for males: category 1: Hgb<14.0; category 2: 14.0≤Hgb<15.0; category 3: 15.0≤Hgb<16.0; category 4: 16.0≤Hgb<17.0; category 5: 17.0≤Hgb<18.0; and category 6: Hgb≥18.0 g/dL. For females, the corresponding classification was as follows: category 1: Hgb<12.0; category 2: 12.0≤Hgb<13.0; category 3: 13.0≤Hgb<14.0; category 4: 14.0≤Hgb<15.0; category 5: 15.0≤Hgb<16.0; and category 6: Hgb≥16.0 g/dL. We decided to set the lower limit of Hgb levels as 14.0 g/dL for male population because research has suggested that the World Health Organization definition of anemia might not be able to distinguish anemic patients with Hgb levels of 13.0-14.0 g/dL [12]. Therefore, we chose a range that would ensure that most anemic patients would be included in the lowest Hgb range in our study. A sex-specific approach to categorization was used because mean serum Hgb levels are different according to sex, making it necessary to separate the exposure variables in this study into sex-specific ranges [9,13] (Supplemental Material 2).
- Statistical Analysis
- We used the chi-square test for categorical variables and analysis of variance for continuous variables to analyze differences in characteristics according to Hgb levels. The associations between Hgb levels and risk of death by various causes were estimated using Cox proportional-hazards models adjusted for potential confounders including age at enrollment, sex, body mass index (BMI), ever smoking (yes, no, and unknown), ever alcohol drinking (yes, no, and unknown), diastolic blood pressure (DBP), blood glucose, serum gamma-glutamyltransferase, and past history of diabetes and hypertension. Not only did these variables show significant differences according to Hgb levels, as presented in Supplemental Material 3, but they were also directly related to all-cause mortality. Cochran-Mantel-Haenszel analysis was used to obtain logit estimates for categories with not enough participants [14].
- We assessed non-linear associations between serum Hgb levels and the respective risk of death by various causes using cubic spline regression models. To evaluate the linearity and non-linearity of these relationships, we calculated overall and non-linear p-values [15,16]. When we visualized a non-linear pattern in an association between Hgb and cause-specific mortality, we additionally stratified the findings by sex. All statistical analyses were conducted in SAS version 9.4 (SAS Institute Inc., Cary, NC, USA) and the cubic spline regression model was performed in R version 3.5.1 (https://cran.r-project.org/bin/windows/base/old/3.5.1/) using the packages sas7bdat, foreign, survival, pspline, dplyr, Greg, and magrittr.
- Ethics Statement
- This research was approved by the Institutional Review Board of Seoul National University Hospital (No. 1901-016-999).
METHODS
- Baseline Characteristics According to Hgb Levels
- In the study population, there were 31 768 deaths by all causes during the follow-up period. Of these deaths, 6502 subjects died due to CVD and 12 386 subjects died from a malignancy (Supplemental Material 4). The participants in category 1 tended to have lower BMI, systolic blood pressure (SBP), and DBP. All the anthropometric and laboratory variables showed significant differences (p<0.01) according to Hgb levels.
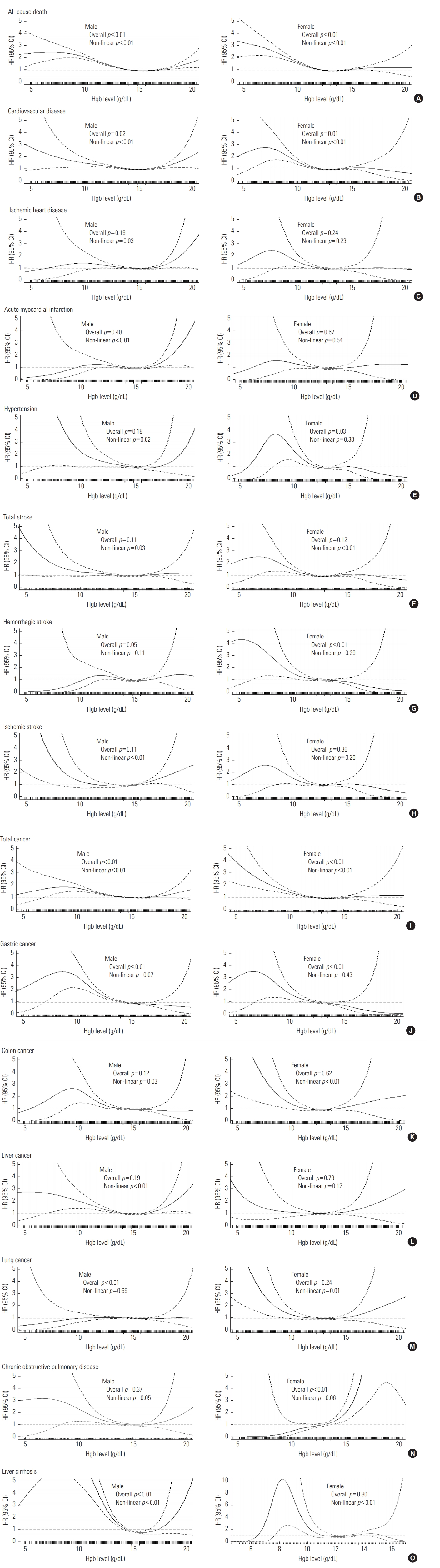
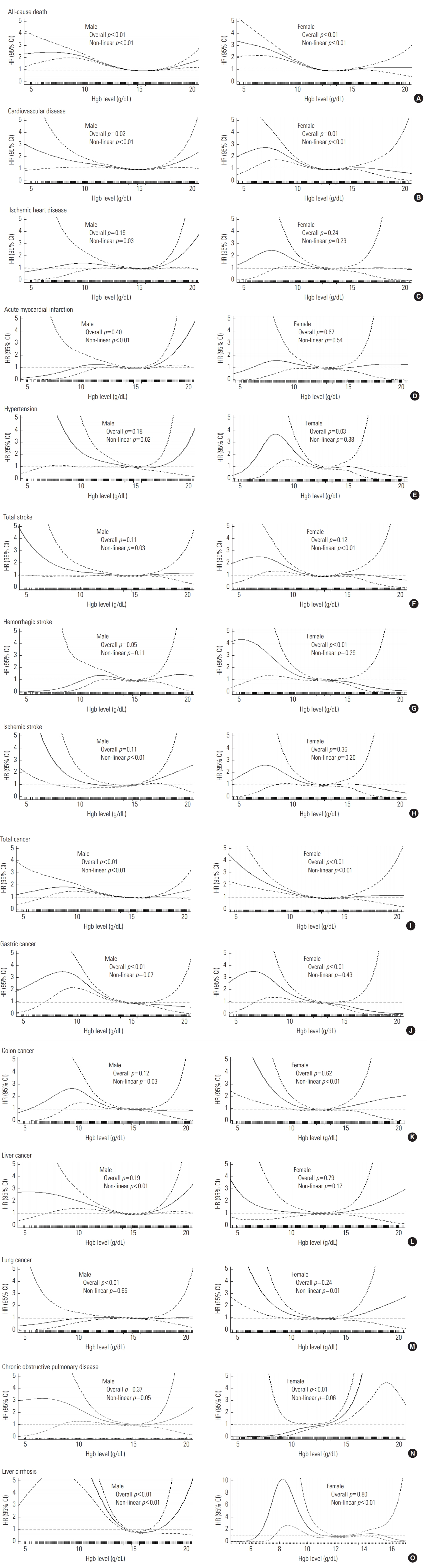
- For all-cause death, CVD death, and total cancer death, the lowest Hgb levels were associated with elevated risk in both males and females, but the specific patterns and relationships in the cubic spline analysis showed discrepancies between males and females (Figure 1).
- All-cause death showed an inverse J-shaped pattern for both males (lowest: hazard ratio [HR], 1.28; 95% confidence interval [CI], 1.23 to 1.32; highest: HR, 1.52; 95% CI, 1.22 to 1.91) and females (lowest: HR, 1.31; 95% CI, 1.23 to 1.39; highest: HR, 1.25; 95% CI, 0.98 to 1.59). The cubic spline analysis confirmed these results, with significant overall and non-linear p-values. For deaths from CVD, a U-shaped association was observed in males (lowest: HR, 1.13; 95% CI, 1.04 to 1.24; highest: HR, 1.77; 95% CI, 1.11 to 2.82), while for females, only the lowest Hgb level showed elevated risk (HR, 1.23; 95% CI, 1.10 to 1.38). The cubic spline graphs for deaths from CVD in males and females also showed a similar pattern to these results. Total cancer death had elevated risk in only the lowest level for both males and females (males: HR, 1.24; 95% CI, 1.17 to 1.31; females: HR, 1.31; 95% CI, 1.18 to 1.45). Although the highest Hgb level for males did not show a significant risk elevation, the cubic spline of total cancer deaths for male population showed a small increased risk at high levels of Hgb, while no such trend was observed for female population. Since all-cause, CVD, and total cancer deaths included many more specific causes of death within each outcome, varying patterns for these outcomes were expected; however, all of them showed significant overall and non-linear p-values.
- When we further evaluated cause-specific deaths, IHD deaths showed a J-shaped association in males (non-linear p<0.05) and AMI deaths also showed J-shaped pattern in males (non-linear p<0.01). For deaths due to hypertension, females showed a negative linear association with Hgb levels (overall p<0.05, non-linear p=0.38). Hemorrhagic stroke deaths yielded a negative linear association in both sexes (overall p=0.05 for males, p<0.01 for females). Both males and females showed a negative linear association between Hgb levels and risk of gastric cancer death (both overall p<0.01). For colon cancer, an inverse J-shaped association was found in both sexes (non-linear p< 0.05 for males, p<0.01 for females; respectively). For liver cancer, male population presented a U-shaped pattern (non-linear p<0.01). For lung cancer, males showed a negative linear association (overall p<0.01), while female population showed an inverse J-shaped pattern (non-linear p=0.01). Lastly, for COPD deaths, males showed a J-shaped pattern (non-linear p=0.05) while females presented a positive linear association (overall p<0.01). Deaths due to liver cirrhosis showed a U-shaped pattern in the male population (non-linear p<0.01).
- Deaths due to IHD and AMI showed significant associations with both the lowest and the highest Hgb levels only in the male population (for lowest level: HR, 1.14; 95% CI, 0.98 to 1.34; HR, 1.16; 95% CI, 0.96 to 1.40; for highest level: HR, 2.87; 95% CI, 1.48 to 5.57; HR, 3.05; 95% CI, 1.44 to 6.48, respectively). For deaths from hypertension, only females presented a negative linear association (lowest level: HR, 1.86; 95% CI, 1.29 to 2.67). For liver cancer, males showed a U-shaped pattern (lowest level: HR, 1.36; 95% CI, 1.18 to 1.56; highest level: HR, 2.11; 95% CI, 1.05 to 4.26). For lung cancer, a negative linear association was found in the male population (lowest level: HR, 1.17; 95% CI, 1.05 to 1.33), while the female population demonstrated an inverse J-shaped pattern (lowest level: HR, 1.25; 95% CI, 0.96 to 1.63; highest level: HR, 2.58; 95% CI, 1.21 to 5.50). For COPD deaths, males showed an inverse J-shaped pattern (lowest level: HR, 1.62; 95% CI, 1.14 to 2.30; highest level: HR, 3.84; 95% CI, 1.22 to 12.13), while a positive linear association was found in females (highest level: HR, 6.60; 95% CI, 2.37 to 18.41). Finally, for deaths from liver cirrhosis, only the male population presented a U-shaped pattern (lowest level: HR, 3.64; 95% CI, 2.49 to 5.33; highest level: HR, 5.97; 95% CI, 1.44 to 24.82). However, some outcome variables showed similar patterns in both males and females. The risk of death from hemorrhagic stroke showed a negative linear association with Hgb levels in males and females (males: HR, 1.31; 95% CI, 1.03 to 1.67; females: HR, 1.29; 95% CI, 0.98 to 1.69, respectively). For site-specific cancer deaths, gastric cancer showed a negative linear association in both sexes (males: HR, 1.37; 95% CI, 1.18 to 1.59; females: HR, 1.44; 95% CI, 1.09 to 1.91). For colon cancer, both males and females presented an inverse J-shaped pattern in the cubic spline analysis, but only the lowest Hgb level for males (HR, 1.24; 95% CI, 1.02 to 1.49) and the highest Hgb level for females (HR, 2.74; 95% CI, 1.12 to 6.72) resulted in significant HRs.
- We performed sensitivity analyses by removing participants with any CVDs, any malignancies, and with either COPD or liver cirrhosis (n=37 127). Among 450 516 healthy individuals, similar patterns according to sex for the risk of death from various causes were observed. In male population, U-shaped, J-shaped, or inverse J-shaped associations between Hgb and the risk of death from IHD, AMI, liver cancer, cirrhosis, and COPD were shown, while the risk of death from hypertension was inversely associated with Hgb levels in females (Tables 1-4) (Supplemental Materials 5-8).
RESULTS
All-cause, cardiovascular, and total cancer mortality according to Hgb levels
Cause-specific mortality according to Hgb levels
Similarities and differences in the associations between Hgb levels and cause-specific mortality according to sex
- Prior epidemiological and biological studies of mechanisms based on sex hormones between males and females can sufficiently explain different patterns in deaths between males and females by Hgb levels. Androgens act as a direct stimulant of the production of red cell mass in the bone marrow and erythropoietin in the kidneys, while estrogen acts as a direct inhibitor of these processes [17-19]. Conversely, estrogen is considered to exhibit an endothelial vasodilator function, impacting the cardiovascular system and resulting in a protective effect from CVDs, whereas androgens induce vasoconstriction [13]. Higher Hgb levels, even within the normal range, are clearly associated with the risk of thrombosis [20]. These previous studies have suggested that the increased risk of IHD, including AMI, in male population is mediated by higher Hgb levels, which increase the possibility of thrombosis and vasoconstriction. In addition, low Hgb levels are well known to increase the risk of IHD, including AMI [20]. Thus, the U-shaped association of Hgb levels with the risk of IHD death in male population can be explained for both higher and lower Hgb values [20,21]. Regarding the risk of death from stroke, a retrospective study showed negative linear associations between Hgb levels and death from stroke in both males and females [6]. However, the association between Hgb levels and stroke death risk was similar between males and females [6].
- In our results, male population presented a negative linear association with lung cancer mortality, while females demonstrated an inverse J-shaped association. Among the many mechanisms that have been suggested to explain sex differences in lung cancer mortality, sex hormones seem to be the most convincing one. Even though the exact mechanism is still unclear, estrogen acts as an estrogen receptor ligand and may promote cell proliferation. Furthermore, strong evidence has been reported that estrogen stimulates angiogenesis, which is the most important target for lung cancer treatment [22,23].
- There are several reasons for sex-specific associations between Hgb levels and the risk for death from specific diseases. Physiologically, healthy males and females have different mean concentrations of Hgb. In particular, Hgb levels are higher in males than in females, and the cut-off levels of anemia are lower for females than for males [17]. Sex differences in Hgb levels are likely to be associated with the risk of death from diseases. The effects of sex hormones on Hgb levels and the vascular system are discussed above. These differences in hormone levels between males and females may play a key role in discrepancies according to sex in our outcome variables. In males, a high risk for death was mainly found for diseases caused by atherosclerosis. Atherosclerosis is linked to thrombosis, the risk of which increases at high Hgb levels, especially in males, and the risks of high blood viscosity have been emphasized in males [17,24]. As shown in Supplemental Material 3, male population with the highest Hgb levels tended to have high mean SBP, DBP, BMI, and blood sugar levels, unlike what was observed for females. They were also more likely to smoke and drink than females, which could also act as risk factors for increased blood viscosity [17]. These differences between males and females in terms of general characteristics indirectly explain the differences in results by sex at the highest Hgb levels. Despite these hormonal differences, the risk of death from some diseases in our results was not affected by sex-specific Hgb levels. Our data contained participants in a health examination program, so there were relatively many participants with the lowest and highest Hgb levels; however, some categories of cause-specific death did not have enough participants to evaluate the effect of sex-specific Hgb levels on mortality.
- In our sensitivity analysis, the patterns found in a healthier sub-population were consistent with those found in the entire study population. This implies that the associations between Hgb levels and risk of cause-specific deaths still existed in healthy participants. Additionally, when we analyzed the population before excluding participants who died within 2 years of baseline, people with low Hgb levels had a higher risk of mortality and those with high Hgb levels had a lower risk of mortality than the final study population (data not shown). Altogether, this might suggest that serum Hgb levels could be a potential biomarker for predicting the risk of mortality not only in the high-risk population, but also in relatively healthy populations.
- There are limitations of our research. First, the causes of death from national death records were not fully confirmed by physicians or electronic medical records, meaning that possible discrepancies between our data and the real cause of death could not be ruled out. However, a recent study concluded that information on death certificates from Statistics Korea were reasonably valid [25]. Second, our data did not contain information on stages of cancer. Third, we could not investigate levels of blood viscosity because our dataset did not contain information on hematocrit. Fourth, possible residual confounders such as history of prescription medications or chemotherapy were not included. Fifth, it is well known that pregnancy can affect Hgb levels in females, but our data did not contain information on pregnancy. According to statistics in Korea, we estimated that 6.0% of 40-year-old to 44-year-old femlaes were pregnant, corresponding to 2906 females in our study, and that 0.2% of 45-year-old to 49-year-old females were pregnant, corresponding to 77 females in our study [26]. Lastly, the method of Hgb sample collection might have differed in various healthcare centers, leading to measurement errors that could have affected our exposure variables.
- Despite the above limitations, our study has strengths. First, we used public data with a large study population to increase generalizability. Second, the follow-up period of our data (up to 11 years) was relatively long.
- Our results both demonstrate the effects of higher and lower levels of Hgb on various types of cause-specific mortality risk and show sex-specific differences in the association between Hgb levels and cause-specific mortality. Moreover, these patterns regarding Hgb levels and the risk of mortality were found in a relatively healthy sub-population, as well as in the entire population of health examinees. This implies that serum Hgb levels could serve as a potential biomarker for predicting the risk of mortality in the healthy population. Further studies are required to expand upon our results.
DISCUSSION
SUPPLEMENTAL MATERIALS
Supplemental Material 1.
Supplemental Material 2.
Supplemental Material 3.
Supplemental Material 4.
Supplemental Material 5.
Supplemental Material 6.
Supplemental Material 7.
Supplemental Material 8.
-
CONFLICT OF INTEREST
The authors have no conflicts of interest associated with the material presented in this paper.
Notes
ACKNOWLEDGEMENTS
-
AUTHOR CONTRIBUTIONS
Conceptualization: SKP, YA. Data curation: YA, SM. Formal analysis: YA. Funding acquisition: SKP. Methodology: SKP, YA, JJ. Project administration: SKP. Visualization: SL, JJ, SM, YA. Writing - original draft: YA, SL, SM. Writing - review & editing: YA, JJ, SKP.
Notes
| Cause of death |
Six levels of Hgb (g/dL) |
||||||
|---|---|---|---|---|---|---|---|
|
|
Lowest (anemia) |
|
Reference |
|
|
Highest |
|
|
Male |
Hgb <14.0 |
14.0-14.9 |
15.0-15.9 |
16.0-16.9 |
17.0-17.9 |
Hgb ≥18.0 |
|
| Female | Hgb <12.0 | 12.0-12.9 | 13.0-13.9 | 14.0-14.9 | 15.0-15.9 | Hgb ≥16.0 | |
| All-cause | |||||||
| Male | 1.28 (1.23, 1.32)* | 1.06 (1.03, 1.10)* | 1.00 (reference) | 1.05 (0.99, 1.10) | 1.13 (1.02, 1.25)* | 1.52 (1.22, 1.91)* | |
| Death (n) | 6927 | 7007 | 5183 | 2126 | 410 | 77 | |
| Female | 1.31 (1.23, 1.39)* | 1.01 (0.96, 1.06) | 1.00 (reference) | 1.02 (0.96, 1.09) | 1.15 (1.02, 1.29)* | 1.25 (0.98, 1.59) | |
| Death (n) | 1820 | 3450 | 3138 | 1265 | 299 | 66 | |
| CVD | |||||||
| Male | 1.13 (1.04, 1.24)* | 1.05 (0.97, 1.14) | 1.00 (reference) | 1.06 (0.95, 1.19) | 1.12 (0.89, 1.41) | 1.77 (1.11, 2.82)* | |
| Death (n) | 1155 | 1298 | 970 | 412 | 80 | 18 | |
| Female | 1.23 (1.10, 1.38)* | 0.92 (0.84, 1.01) | 1.00 (reference) | 0.95 (0.84, 1.08) | 1.08 (0.85, 1.36) | 1.13 (0.69, 1.85) | |
| Death (n) | 468 | 856 | 834 | 318 | 77 | 16 | |
| IHD | |||||||
| Male | 1.14 (0.98, 1.34) | 1.08 (0.93, 1.25) | 1.00 (reference) | 1.00 (0.81, 1.23) | 1.06 (0.70, 1.60) | 2.87 (1.48, 5.57)* | |
| Death (n) | 343 | 416 | 309 | 124 | 24 | 9 | |
| Female | 1.08 (0.84, 1.38) | 0.97 (0.80, 1.19) | 1.00 (reference) | 0.78 (0.58, 1.05) | 1.16 (0.72, 1.86) | 0.61 (0.15, 2.47) | |
| Death (n) | 93 | 203 | 188 | 59 | 19 | 2 | |
| AMI | |||||||
| Male | 1.16 (0.96, 1.40) | 1.12 (0.94, 1.33) | 1.00 (reference) | 1.06 (0.83, 1.34) | 1.20 (0.76, 1.89) | 3.05 (1.44, 6.48)* | |
| Death (n) | 249 | 313 | 227 | 97 | 20 | 7 | |
| Female | 0.94 (0.70, 1.27) | 1.01 (0.80, 1.27) | 1.00 (reference) | 0.82 (0.59, 1.14) | 1.31 (0.78, 2.20) | 0.41 (0.06, 2.96) | |
| Death (n) | 63 | 160 | 141 | 46 | 16 | 1 | |
| Hypertension | |||||||
| Male | 1.16 (0.81, 1.67) | 1.01 (0.71, 1.45) | 1.00 (reference) | 0.77 (0.45, 1.33) | 0.72 (0.23, 2.31) | 3.18 (0.78, 13.06) | |
| Death (n) | 71 | 71 | 54 | 17 | 3 | 2 | |
| Female | 1.86 (1.29, 2.67)* | 0.96 (0.68, 1.35) | 1.00 (reference) | 1.03 (0.66, 1.62) | 1.21 (0.55, 2.64) | 0.92 (0.13, 6.66) | |
| Death (n) | 57 | 69 | 64 | 27 | 7 | 1 | |
Values are presented as hazard ratio (95% confidence interval).
Hgb, hemoglobin; CVD, cardiovascular disease; IHD, ischemic heart disease; AMI, acute myocardial infarction.
1 Adjusted for age, body mass index, cigarette smoking, alcohol drinking, exercise, diastolic blood pressure, blood glucose levels, and gamma-glutamyltransferase levels.
* p<0.05.
| Cause of death |
Six levels of Hgb (g/dL) |
||||||
|---|---|---|---|---|---|---|---|
|
|
Lowest (anemia) |
|
Reference |
|
|
Highest |
|
|
Male |
Hgb <14.0 |
14.0-14.9 |
15.0-15.9 |
16.0-16.9 |
17.0-17.9 |
Hgb ≥18.0 |
|
| Female | Hgb <12.0 | 12.0-12.9 | 13.0-13.9 | 14.0-14.9 | 15.0-15.9 | Hgb ≥16.0 | |
| Stroke | |||||||
| Male | 1.09 (0.96, 1.24) | 0.99 (0.88, 1.13) | 1.00 (reference) | 1.07 (0.90, 1.27) | 1.08 (0.77, 1.52) | 1.03 (0.43, 2.48) | |
| Death (n) | 554 | 586 | 452 | 192 | 36 | 5 | |
| Female | 1.17 (1.00, 1.38) | 0.91 (0.80, 1.04) | 1.00 (reference) | 0.93 (0.77, 1.11) | 1.07 (0.77, 1.48) | 1.22 (0.63, 2.36) | |
| Death (n) | 227 | 438 | 436 | 161 | 40 | 9 | |
| Hemorrhagic stroke | |||||||
| Male | 1.31 (1.03, 1.67)* | 1.21 (0.96, 1.52) | 1.00 (reference) | 1.10 (0.81, 1.51) | 1.55 (0.91, 2.65) | 1.49 (0.37, 6.04) | |
| Death (n) | 149 | 183 | 127 | 58 | 15 | 2 | |
| Female | 1.29 (0.98, 1.69) | 0.92 (0.73, 1.15) | 1.00 (reference) | 0.89 (0.65, 1.21) | 0.55 (0.26, 1.17) | 0.79 (0.20, 3.20) | |
| Death (n) | 83 | 149 | 153 | 54 | 7 | 2 | |
| Ischemic stroke | |||||||
| Male | 1.01 (0.81, 1.26) | 0.93 (0.75, 1.16) | 1.00 (reference) | 1.40 (1.06, 1.84)* | 1.35 (0.78, 2.34) | 1.27 (0.31, 5.13) | |
| Death (n) | 184 | 181 | 143 | 78 | 14 | 2 | |
| Female | 1.19 (0.88, 1.60) | 0.93 (0.72, 1.19) | 1.00 (reference) | 0.91 (0.65, 1.29) | 1.21 (0.68, 2.14) | 0.96 (0.24, 3.86) | |
| Death (n) | 70 | 131 | 123 | 45 | 13 | 2 | |
| Cause of death |
Six levels of Hgb (g/dL) |
||||||
|---|---|---|---|---|---|---|---|
|
|
Lowest (anemia) |
|
Reference |
|
|
Highest |
|
|
Male |
Hgb <14.0 |
14.0-14.9 |
15.0-15.9 |
16.0-16.9 |
17.0-17.9 |
Hgb ≥18.0 |
|
| Female | Hgb <12.0 | 12.0-12.9 | 13.0-13.9 | 14.0-14.9 | 15.0-15.9 | Hgb ≥16.0 | |
| Total cancers | |||||||
| Male | 1.24 (1.17, 1.31)* | 1.07 (1.01, 1.13)* | 1.00 (reference) | 1.03 (0.96, 1.18) | 1.09 (0.93, 1.28) | 1.29 (0.89, 1.88) | |
| Death (n) | 2764 | 2994 | 2238 | 911 | 171 | 28 | |
| Female | 1.31 (1.18, 1.45)* | 1.07 (0.98, 1.16) | 1.00 (reference) | 0.99 (0.88, 1.11) | 1.13 (0.92, 1.40) | 1.17 (0.75, 1.82) | |
| Death (n) | 556 | 1162 | 1041 | 406 | 95 | 20 | |
| Gastric cancer | |||||||
| Male | 1.37 (1.18, 1.59)* | 0.99 (0.85, 1.15) | 1.00 (reference) | 0.89 (0.72, 1.11) | 0.67 (0.40, 1.12) | 0.96 (0.31, 2.98) | |
| Death (n) | 435 | 398 | 322 | 113 | 15 | 3 | |
| Female | 1.44 (1.09, 1.91)* | 1.04 (0.82, 1.32) | 1.00 (reference) | 0.82 (0.58, 1.17) | 0.99 (0.52, 1.88) | 1.31 (0.21, 6.51)2 | |
| Death (n) | 82 | 147 | 130 | 41 | 10 | 0 | |
| Colon cancer | |||||||
| Male | 1.24 (1.02, 1.49)* | 1.02 (0.85, 1.22) | 1.00 (reference) | 1.01 (0.79, 1.30) | 0.71 (0.39, 1.30) | 1.38 (0.44, 4.30) | |
| Death (n) | 246 | 266 | 213 | 87 | 11 | 3 | |
| Female | 1.06 (0.76, 1.47) | 1.08 (0.84, 1.39) | 1.00 (reference) | 1.05 (0.75, 1.47) | 1.33 (0.73, 2.41) | 2.74 (1.12, 6.72)* | |
| Death (n) | 53 | 136 | 117 | 47 | 12 | 5 | |
| Liver cancer | |||||||
| Male | 1.36 (1.18, 1.56)* | 1.06 (0.92, 1.20) | 1.00 (reference) | 1.19 (1.01, 1.41)* | 1.50 (1.10, 2.04)* | 2.11 (1.05, 4.26)* | |
| Death (n) | 446 | 494 | 403 | 200 | 45 | 8 | |
| Female | 1.10 (0.80, 1.52) | 1.01 (0.79, 1.29) | 1.00 (reference) | 1.00 (0.72, 1.38) | 1.33 (0.77, 2.32) | 0.93 (0.23, 3.77) | |
| Death (n) | 56 | 131 | 126 | 51 | 14 | 2 | |
| Lung cancer | |||||||
| Male | 1.17 (1.05, 1.33)* | 1.06 (0.95, 1.17) | 1.00 (reference) | 0.96 (0.82, 1.12) | 0.99 (0.71, 1.36) | 0.88 (0.37, 2.13) | |
| Death (n) | 767 | 862 | 612 | 219 | 39 | 5 | |
| Female | 1.25 (0.96, 1.63) | 1.10 (0.89, 1.35) | 1.00 (reference) | 1.02 (0.77, 1.36) | 0.82 (0.44, 1.50) | 2.58 (1.21, 5.50)* | |
| Death (n) | 86 | 199 | 168 | 67 | 11 | 7 | |
| Cause of death |
Six levels of Hgb (g/dL) |
||||||
|---|---|---|---|---|---|---|---|
|
|
Lowest (anemia) |
|
Reference |
|
|
Highest |
|
|
Male |
Hgb <14.0 |
14.0-14.9 |
15.0-15.9 |
16.0-16.9 |
17.0-17.9 |
Hgb ≥18.0 |
|
| Female | Hgb <12.0 | 12.0-12.9 | 13.0-13.9 | 14.0-14.9 | 15.0-15.9 | Hgb ≥16.0 | |
| COPD | |||||||
| Male | 1.62 (1.14, 2.30)* | 1.14 (0.88, 1.47) | 1.00 (reference) | 0.96 (0.74, 1.24) | 0.82 (0.30, 2.22) | 3.84 (1.22, 12.13)* | |
| Death (n) | 174 | 166 | 91 | 48 | 4 | 3 | |
| Female | 0.70 (0.41, 1.19) | 0.77 (0.50, 1.17) | 1.00 (reference) | 1.12 (0.64, 1.96) | 2.49 (1.17, 5.30)* | 6.60 (2.37, 18.41)* | |
| Death (n) | 21 | 44 | 43 | 17 | 8 | 4 | |
| Liver cirrhosis | |||||||
| Male | 3.64 (2.49, 5.33)* | 1.73 (1.17, 2.57)* | 1.00 (reference) | 1.22 (0.70, 2.13) | 2.55 (1.14, 5.72)* | 5.97 (1.44, .24.82)* | |
| Death (n) | 117 | 75 | 37 | 20 | 7 | 2 | |
| Female | 1.10 (0.61, 2.00) | 0.52 (0.29, 0.92) | 1.00 (reference) | 0.99 (0.52, 1.88) | 0.73 (0.17, 3.05) | 4.89 (0.75, 26.67)2 | |
| Death (n) | 19 | 19 | 32 | 13 | 2 | 0 | |
Values are presented as hazard radio (95% confidence interval).
Hgb, hemoglobin; COPD, chronic obstructive pulmonary disease.
1 Adjusted for age, body mass index, cigarette smoking, alcohol drinking, exercise, diastolic blood pressure, blood glucose levels, and gamma-glutamyltransferase levels.
2 Logit estimates not available.
* p<0.05.
- 1. Caro JJ, Salas M, Ward A, Goss G. Anemia as an independent prognostic factor for survival in patients with cancer: a systemic, quantitative review. Cancer 2001;91(12):2214-2221ArticlePubMed
- 2. Zakai NA, Katz R, Hirsch C, Shlipak MG, Chaves PH, Newman AB, et al. A prospective study of anemia status, hemoglobin concentration, and mortality in an elderly cohort: the Cardiovascular Health Study. Arch Intern Med 2005;165(19):2214-2220ArticlePubMed
- 3. Kalra PR, Greenlaw N, Ferrari R, Ford I, Tardif JC, Tendera M, et al. Hemoglobin and change in hemoglobin status predict mortality, cardiovascular events, and bleeding in stable coronary artery disease. Am J Med 2017;130(6):720-730ArticlePubMed
- 4. Zhang YH, Lu Y, Lu H, Zhang MW, Zhou YM, Li XL, et al. Pre-treatment hemoglobin levels are an independent prognostic factor in patients with non-small cell lung cancer. Mol Clin Oncol 2018;9(1):44-49ArticlePubMedPMC
- 5. Nissenson AR, Goodnough LT, Dubois RW. Anemia: not just an innocent bystander? Arch Intern Med 2003;163(12):1400-1404ArticlePubMed
- 6. Kimberly WT, Lima FO, O’Connor S, Furie KL. Sex differences and hemoglobin levels in relation to stroke outcomes. Neurology 2013;80(8):719-724ArticlePubMedPMC
- 7. Di Carlo A, Lamassa M, Baldereschi M, Pracucci G, Basile AM, Wolfe CD, et al. Sex differences in the clinical presentation, resource use, and 3-month outcome of acute stroke in Europe: data from a multicenter multinational hospital-based registry. Stroke 2003;34(5):1114-1119ArticlePubMed
- 8. Kapral MK, Fang J, Hill MD, Silver F, Richards J, Jaigobin C, et al. Sex differences in stroke care and outcomes: results from the Registry of the Canadian Stroke Network. Stroke 2005;36(4):809-814ArticlePubMed
- 9. Murphy WG. The sex difference in haemoglobin levels in adults - mechanisms, causes, and consequences. Blood Rev 2014;28(2):41-47ArticlePubMed
- 10. Seong SC, Kim YY, Park SK, Khang YH, Kim HC, Park JH, et al. Cohort profile: the National Health Insurance Service-National Health Screening Cohort (NHIS-HEALS) in Korea. BMJ Open 2017;7(9):e016640ArticlePubMedPMC
- 11. Weiss G, Goodnough LT. Anemia of chronic disease. N Engl J Med 2005;352(10):1011-1023ArticlePubMed
- 12. Beutler E, Waalen J. The definition of anemia: what is the lower limit of normal of the blood hemoglobin concentration? Blood 2006;107(5):1747-1750ArticlePubMedPMCPDF
- 13. Miller VM, Duckles SP. Vascular actions of estrogens: functional implications. Pharmacol Rev 2008;60(2):210-241ArticlePubMedPMC
- 14. Rayner JC, Best DJ. Unconditional analogues of Cochran–Mantel–Haenszel tests. Aust N Z J Stat 2017;59(4):485-494Article
- 15. Knafl GJ, Barakat LP, Hanlon AL, Hardie T, Knafl KA, Li Y, et al. Adaptive modeling: an approach for incorporating nonlinearity in regression analyses. Res Nurs Health 2017;40(3):273-282ArticlePubMed
- 16. Kong D, Ibrahim JG, Lee E, Zhu H. FLCRM: functional linear cox regression model. Biometrics 2018;74(1):109-117ArticlePubMed
- 17. Garvin JH. Sex-specific aspects of pediatric hematology and oncology. In: Legato MJ, editor. Principles of gender-specific medicine. 2nd ed. Amsterdam: Elsevier; 2010. p. 51-61
- 18. Jelkmann W. Regulation of erythropoietin production. J Physiol 2011;589(6):1251-1258ArticlePubMed
- 19. Shahani S, Braga-Basaria M, Maggio M, Basaria S. Androgens and erythropoiesis: past and present. J Endocrinol Invest 2009;32(8):704-716ArticlePubMedPDF
- 20. Danesh J, Collins R, Peto R, Lowe GD. Haematocrit, viscosity, erythrocyte sedimentation rate: meta-analyses of prospective studies of coronary heart disease. Eur Heart J 2000;21(7):515-520ArticlePubMedPDF
- 21. Stucchi M, Cantoni S, Piccinelli E, Savonitto S, Morici N. Anemia and acute coronary syndrome: current perspectives. Vasc Health Risk Manag 2018;14: 109-118ArticlePubMedPMC
- 22. Kiyohara C, Ohno Y. Sex differences in lung cancer susceptibility: a review. Gend Med 2010;7(5):381-401ArticlePubMed
- 23. Shimada S, Hasegawa K, Wada H, Terashima S, Satoh-Asahara N, Yamakage H, et al. High blood viscosity is closely associated with cigarette smoking and markedly reduced by smoking cessation. Circ J 2011;75(1):185-189ArticlePubMed
- 24. Gagnon DR, Zhang TJ, Brand FN, Kannel WB. Hematocrit and the risk of cardiovascular disease--the Framingham study: a 34-year follow-up. Am Heart J 1994;127(3):674-682ArticlePubMed
- 25. Shin HY, Lee JY, Kim JE, Lee S, Youn H, Kim H, et al. Cause-of-death statistics in 2016 in the Republic of Korea. J Korean Med Assoc 2018;61(9):573-584Article
- 26. Korean Statistical Information Service. National estimate population. 2017 [cited 2019 Jan 30]. Available from: http://kosis.kr/publication/publicationThema.do?pubcode=CC(Korean)
REFERENCES
Figure & Data
References
Citations
- Cross-phenotype association analysis of gastric cancer: in-silico functional annotation based on the disease–gene network
Sangjun Lee, Han-Kwang Yang, Hyuk-Joon Lee, Do Joong Park, Seong-Ho Kong, Sue K. Park
Gastric Cancer.2023; 26(4): 517. CrossRef - 1H-NMR metabolomics-based surrogates to impute common clinical risk factors and endpoints
D. Bizzarri, M.J.T. Reinders, M. Beekman, P.E. Slagboom, BBMRI-NL, E.B. van den Akker
eBioMedicine.2022; 75: 103764. CrossRef - Coronary Atherosclerotic Disease and Cancer: Risk Factors and Interrelation
Jinjing Li, Jieqiong Zhao, Yonghong Lei, Yan Chen, Miaomiao Cheng, Xiaoqing Wei, Jing Liu, Pengyun Liu, Ruirui Chen, Xiaoqing Yin, Lei Shang, Xue Li
Frontiers in Cardiovascular Medicine.2022;[Epub] CrossRef - Binary cutpoint and the combined effect of systolic and diastolic blood pressure on cardiovascular disease mortality: A community-based cohort study
Ju-Yeun Lee, Ji Hoon Hong, Sangjun Lee, Seokyung An, Aesun Shin, Sue K. Park, Tariq Jamal Siddiqi
PLOS ONE.2022; 17(6): e0270510. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite