Teachers’ Negative Attitudes and Limited Health Literacy Levels as Risks for Low Awareness of Epilepsy in Turkey
Article information

Abstract
Objectives
For students with epilepsy, schools are a critical environment for managing the disease properly. This study examined awareness of epilepsy, attitudes toward epilepsy, and health literacy among school teachers in Turkey.
Methods
This study was conducted in a city in Turkey with 1408 public school teachers from June 2021 to September 2021.
Results
The median scores of the scales were 5, 29, and 32 for epilepsy awareness, epilepsy attitudes, and health literacy, respectively. Epilepsy awareness was higher in women, and epilepsy attitudes were more positive in women than men (p<0.05). While epilepsy awareness was higher in primary school teachers, epilepsy attitudes were more positive in secondary school teachers (p<0.05). Epilepsy awareness was lower in secondary school teachers (odds ratio [OR], 1.27; p<0.05), those who did not have an individual with epilepsy in their family/social environment (OR, 1.57; p<0.001), those who did not have a student with epilepsy in their class (OR, 1.45; p<0.05), and in those who had not witnessed an epilepsy seizure (OR,1.19; p<0.05). Compared to those with positive attitudes regarding epilepsy, epilepsy awareness was 1.36 times lower in those with negative attitudes (p<0.001). Epilepsy awareness was 1.92 times lower in those with limited health literacy than those with adequate health literacy (p<0.001).
Conclusions
In this study, low epilepsy awareness, negative epilepsy attitudes, and limited health literacy were common among teachers. The findings from this study suggest that panels, workshops, and health training on epilepsy should be organized for school teachers and included at regular intervals in certified first-aid practices.
INTRODUCTION
Epilepsy, often neglected as a burden on the public health agenda, is a common neurological disease affecting approximately 50 million people of all ages worldwide. The global prevalence is estimated to be 7.6 cases per 1000 people [1]. The prevalence of epilepsy in Turkey varies between 4 and 5 cases per 1000 people [2,3].
Although epilepsy is one of the most common chronic diseases, it is often unfamiliar to the public. Individuals with epilepsy are targeted by social stigma and discrimination, which may reflect cultural differences in public awareness and attitudes towards the disease. General misperceptions are clustered in terms of causes, prognosis, treatment of epilepsy, and first aid measures during an epileptic seizure [4].
Epilepsy is a disease characterized by seizures and involuntary movements caused by the abnormally high electrical activity of neurons in the brain. Such aberrant activity can result in a broad spectrum of activity, from convulsions to a phenomenon that may come and go unnoticed within a few seconds [5]. False and inaccurate perceptions that the disease is a form of insanity, contagious, and incurable lead to stigma [1].
People with epilepsy are prone to post-seizure physical injuries [6]. First aid measures aim to prevent harm to people with epilepsy during a seizure. Lack of awareness and misunderstandings about first aid measures affect the likelihood of someone taking helpful or harmful measures while witnessing a seizure [7].
The complexity of epilepsy and the diverse cultural perceptions associated with the disease have led to the need to promote awareness of epilepsy in the general population, particularly among groups with limited health literacy (HL) [8]. HL pertains to people’s knowledge and competencies to meet complex health demands in modern societies [9].
As a social determinant of health, HL has become a critical skill for today’s societies in disease prevention, control, receiving healthcare, and benefiting from health services [10]. Studies conducted in different countries have reported that teachers’ HL levels were limited [11,12]. A similar situation holds true for Turkish teachers [13]. As in other chronic diseases, it is expected that the family, the whole society, and the patient should be health-literate in managing epilepsy [7,14-16].
Children and young people with epilepsy are exposed to incorrect views in social settings such as school. Students may experience difficulties adapting to school, learning, and interacting socially. These difficulties may be caused not only by epilepsy itself but also by their teachers’ attitudes and expectations [17].
Schools must increase knowledge and awareness about epilepsy to reduce stigma and improve negative attitudes towards the disease. In addition, it is necessary to determine teachers’ training needs and evaluate their first aid skills. Starting public health interventions with school teachers will raise awareness among students and society. The steps that improve the HL of teachers will also provide support for developing epilepsy awareness (EAW) and improving the disease’s management in educational environments.
Research Problems
(1) What is the level of EAW among teachers?; (2) What is the level of epilepsy attitudes (EAT) among teachers?; (3) What is the level of HL among teachers?; (4) Is the EAW of teachers related to socio-demographic factors?; and (5) Is EAW among teachers related to EAT and HL?
Hypothesis of the Study
There are relationships among EAW, socio-demographic factors, EAT, and HL.
This study examined EAW, EAT toward epilepsy, and HL among school teachers.
METHODS
Study Design
This descriptive, correlational study was conducted in Çorum Province, Turkey from June 2021 to September 2021. The research universe consisted of 3800 teachers working in public schools in the city center. HL level in adults was taken as a reference to determine the sample size in the study [18]. According to the current literature, adequate HL was considered to be 30% with a 5% margin of error. The sample size was 1417 with a 95% confidence interval and 80% power. The study included 1408 teachers who could be reached.
Data Collection Tools
Research data were collected using a socio-demographic data form prepared by the researchers, an EAW scale, an EAT scale, and an HL scale.
Socio-demographic Form
The form consisted of 9 questions to determine teachers’ socio-demographic characteristics. The questions included age, sex, marital status, educational level, type of institution, years of experience, presence of chronic disease, existence of people with epilepsy among family and friends, presence of students with epilepsy in the class, and history of witnessing people with epileptic seizures. The questions about the disease were asked to determine the teachers’ awareness of epilepsy.
Epilepsy Awareness Scale
Teachers were asked 12 questions to determine their awareness of the disease’s characteristics, treatability, causes, and first aid practices. One point was awarded for each correct answer. Higher scores indicated greater awareness. In this study, according to the median score (5 points), EAW was categorized into two groups: high awareness (≥5 points) and low awareness (<5 points).
Society’s Attitudes Towards Epilepsy Scale
The scale developed by Lim et al. [6] is grouped into 2 areas, general and personal, and consists of 14 items. The general area comprises 9 items, and the personal area comprises 5 items. The general area addresses general attitudes towards epilepsy, while the personal area asks the participant to consider personal life issues such as marriage and employment. Each item is scored on a 5-point Likert scale where “strongly agree” is given 1 point, and “strongly disagree” is given 5 points. Items 2, 5, 10, 11, and 14 on the scale are scored inversely. The higher the score obtained from the scale, the more negative the attitude [6]. In this study, the Turkish version of the scale [19] was used (Supplemental Material 1), and according to the median value, the EAT score was divided into positive (<29 points) and negative attitudes (≥29 points).
European Health Literacy Scale
This study used the Turkish version of the European Health Literacy Scale (HLS-EU). The 47-item self-report scale was developed to assess HL in people aged ≥15 years. On the scale, 0 indicates the lowest HL level, and 50 indicates the highest level. The formula (Index=[Average−1]×50/3) is used to evaluate the scale [20]. The Turkish version of the scale was used in this study [21] (Supplemental Material 2). Using the median value as a cut-off, a score of <32 points was considered to indicate a limited HL level.
Statistical Analysis
The data were analyzed using SPSS version 22 (IBM Corp., Armonk, NY, USA). During the data analysis, the frequency was used for categorical variables (number, percentage, chi-square test), and descriptive statistics (mean, standard deviation, and median) were used for quantitative variables.
This study’s outcome variable was EAW, divided into two categories (low and high) according to the median score. The association with HL and EAT was subsequently analyzed using the chi-square test.
First, on a binary scale, EAT was classified into negative and positive categories, and an association with socio-demographic factors on EAW was shown. Furthermore, since the HL scores were classified into 2 categories, associations among socio-demographic factors and HL (limited and adequate) were analyzed. The subsequent analyses used multivariate models to assess the mutual influence among EAT, HL, EAW, and other socio-demographic variables. In the analysis, the significance level was set at 0.05.
Ethics Statement
The study was approved by the Ethics Committee of Hitit University (2022-89).
RESULTS
Descriptive Characteristics of the Participants
In the study group, 44.7% of the participants were between 35 years and 44 years old, with a mean age of 43 years; 48.9% of the participants were females and 70.9% were working in primary schools. While the rate of individuals with epilepsy in their family/social environment was 10.9%, the rate of students with epilepsy in their classroom was 17.0%, and 35.4% of the teachers stated that they had witnessed a seizure in individuals who experienced epileptic seizures. The socio-demographic characteristics of the participants are given in Table 1.
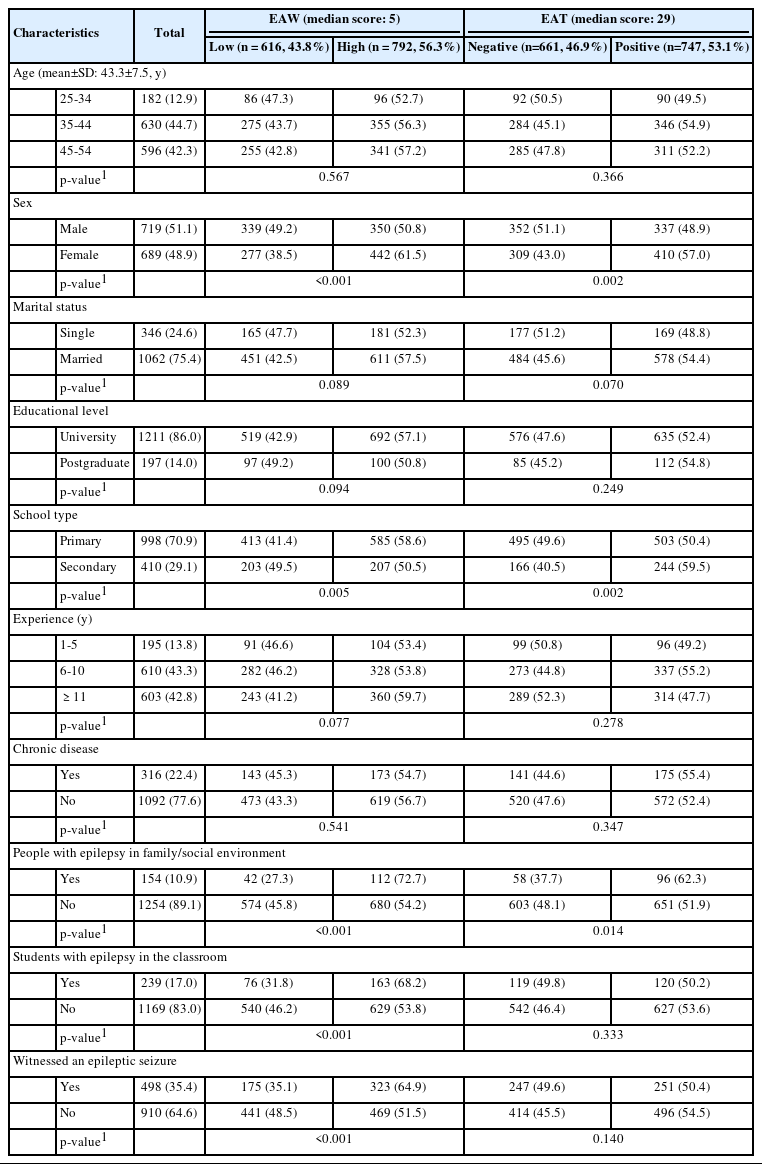
EAW and EAT according to socio-demographic characteristics
EAW was high in 56.3% and low in 43.8% of the participants. EAT was positive in 53.1% and negative in 46.9% of the participants. For HL, 47.4% of participants showed an adequate level, whereas 52.6% had a limited HL level.
Table 1 shows EAW and EAT according to participants’ socio-demographic characteristics. A statistically significant difference in EAW and EAT was found according to sex: 61.5% of female had high EAW scores, compared to 50.8% of male (p<0.001), and 57.0% of female had a positive EAT score, compared to 48.9% of male (p<0.05). Epilepsy awareness showed a statistically significant difference according to the teachers’ institutional types. Whereas 58.6% of primary school teachers had a high EAW, this rate was 50.5% among secondary school teachers (p<0.05). Positive EAT was the highest among secondary school teachers with a result of 59.5% (p<0.05). Among those who had individuals with epilepsy in their family/social environment, EAW and positive EAT were significantly higher, with scores of 72.7% (p<0.001) and 62.3% (p<0.05), respectively. EAW was significantly higher in 68.2% of those who had students with epilepsy in their class and 64.9% of those who had witnessed an epileptic seizure (p<0.001). In this study, EAW and EAT did not differ significantly regarding age, marital status, educational level, seniority, or chronic disease (p>0.05).
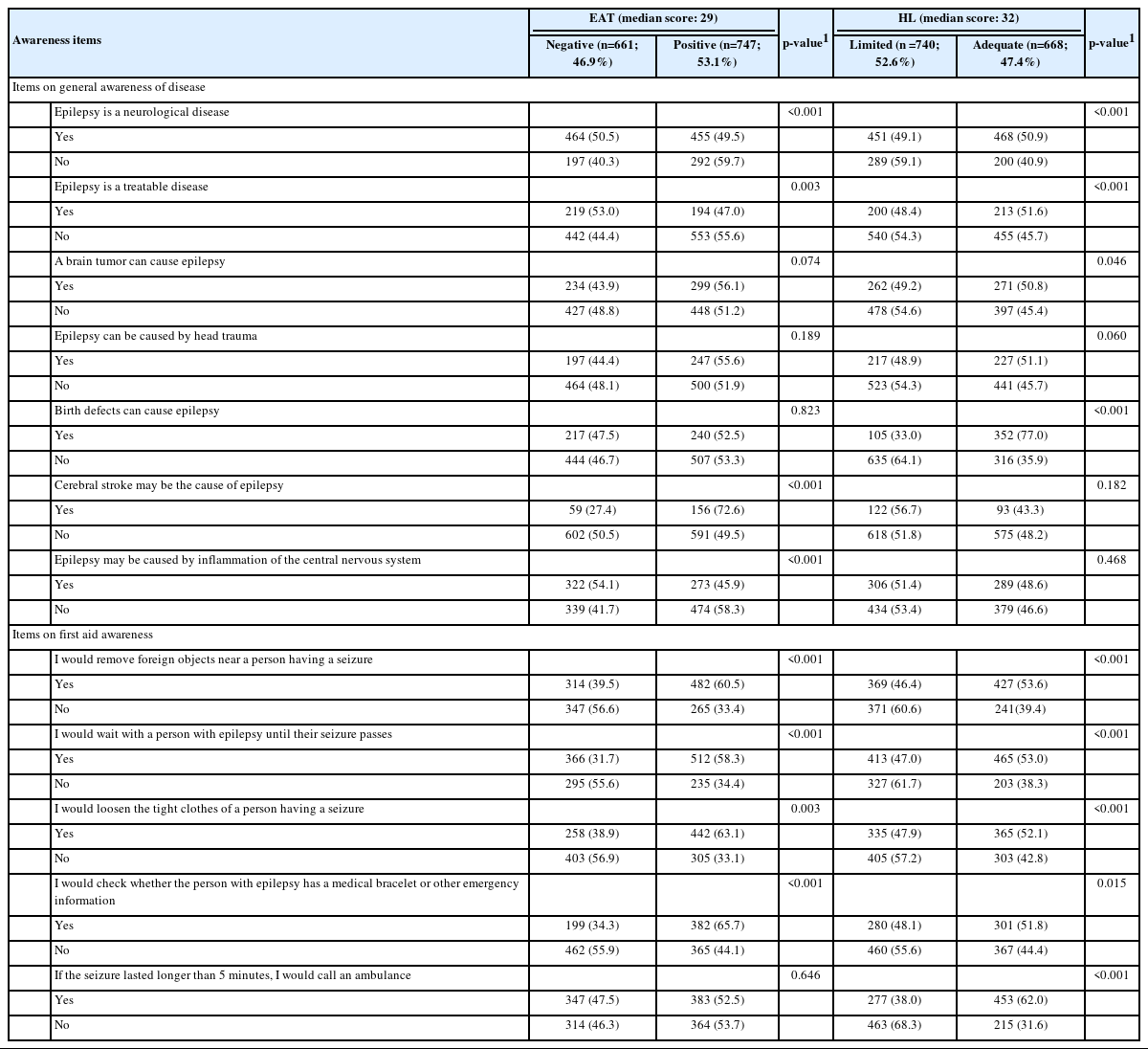
Table 2 shows the EAT and HL levels of the participants according to EAW. Among those who answered “no” to the question of whether epilepsy is a neurological disease, 59.7% had a positive attitude towards epilepsy (p<0.001), while 59.1% had significantly more limited HL (p<0.001). Among those who answered “no” to the question of whether epilepsy is a treatable disease, 55.6% had a positive attitude towards epilepsy (p<0.05), while 54.3% had limited HL (p<0.001). HL levels were significantly adequate for 50.8% of those who stated that epilepsy may develop due to brain tumors (p<0.05), as well as for 77.0% of those who stated that epilepsy may develop due to a congenital defect (p<0.001). EAW was more positive in 72.6% of those who stated that cerebral ischemia could cause epilepsy (p<0.001). EAT was more negative in 54.1% of those who stated that central nervous system inflammation could cause epilepsy (p<0.001).
HL levels and EATs according to epilepsy awareness
It was observed that participants’ awareness of first aid practices differed significantly in terms of EAT and HL. Among those who answered “no” to the question of whether they would remove foreign objects near a person having a seizure, 56.6% had a negative EAT, and 60.6% had a more limited level of HL (p<0.001). Among those who answered “no” to the question, “I would wait with a person with epilepsy until their seizure passes,” 55.6% had a strongly negative EAT, while 61.7% had a higher rate of limited HL (p<0.001). The answer “yes” to the question, “I would loosen the tight clothes of the person having a seizure,” was found to indicate a more positive EAT in 63.1% of participants, and HL was found to be adequate in 52.1% (p<0.001). Among those who answered “yes” to the question, “I would check whether the person with epilepsy has a medical bracelet or other emergency information,” 65.7% had a more positive EAT (p<0.001), and 51.8% had adequate HL (p<0.05). HL was found to be adequate in 62.0% of those who answered “yes” to the question, “If the seizure lasted longer than 5 minutes, I would call an ambulance” (p<0.001).
Table 3 shows the results of the multiple regression analysis of factors associated with low EAW. First, in a binary regression analysis the relationships among socio-demographic factors, EAT, and HL were determined. Positive EAT scores were 1.06 times higher and adequate HL scores were 1.44 times higher in female than in male (p<0.05). Among secondary school teachers, positive EAT scores were 1.46 times higher and adequate HL scores were 1.17 times higher (p<0.05). Positive EAT scores were 1.27 times higher and adequate HL scores were 1.11 times higher in those who had individuals with epilepsy in their family/social environment (p<0.05). In the multiple logistic regression, EAW was 1.27 times lower in secondary school teachers than primary school teachers (p<0.05) and 1.57 times lower in those who did not have individuals with epilepsy in their family/social environment compared to those who did (p<0.001). Furthermore, EAW was 1.45 times lower in those who did not have a student with epilepsy in their class, 1.19 times lower in those who had not witnessed an epileptic seizure (p<0.05), 1.36 times lower in those with a negative EAT than those with a positive EAT (p<0.001), and 1.92 times lower in those with limited HL than those with adequate HL (p<0.001).
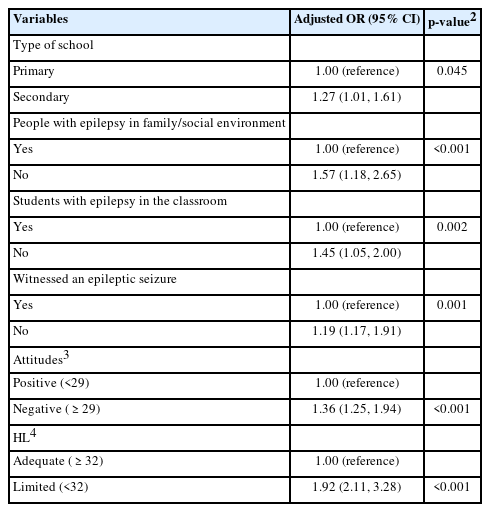
Figure 1 shows the positions of 4 groups of variables (some demographic characteristics, EAW, EAT, and HL) in relation to each other. Figure 2 shows the dimensions of EAT and HL according to EAW. In both figures, teachers’ EAW scores are shown to differ in terms of socio-demographic factors, EAT, and HL.
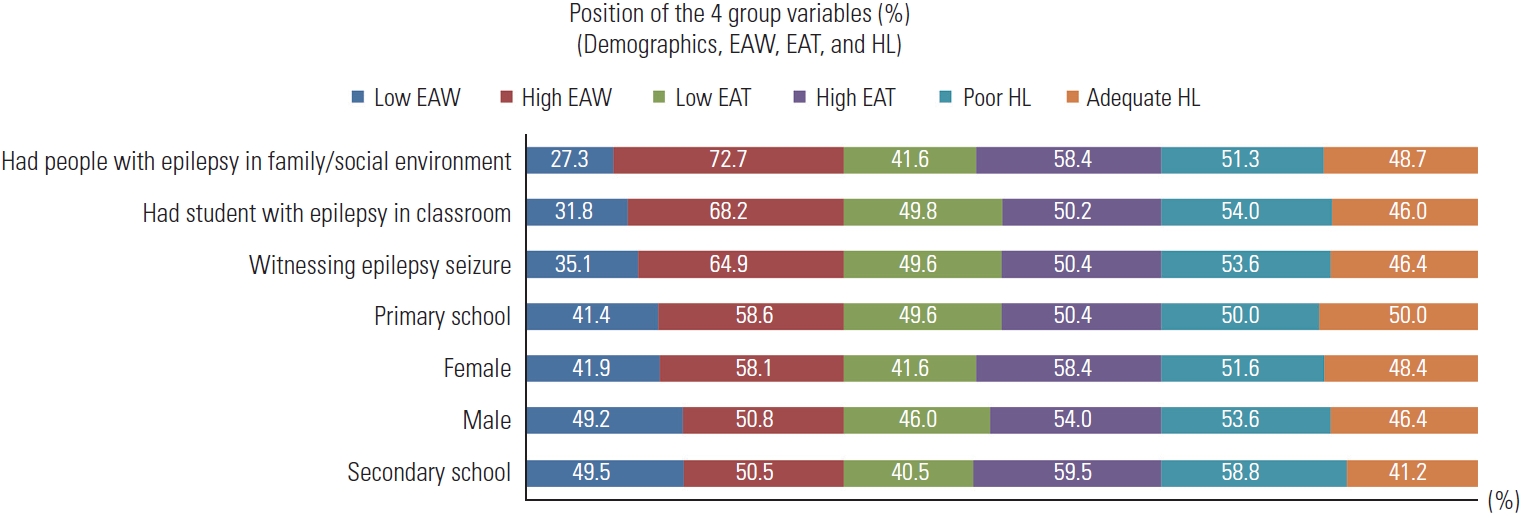
Relative positions of the 4 group variables. EAW, epilepsy awareness; EAT, epilepsy attitudes; HL, health literacy.
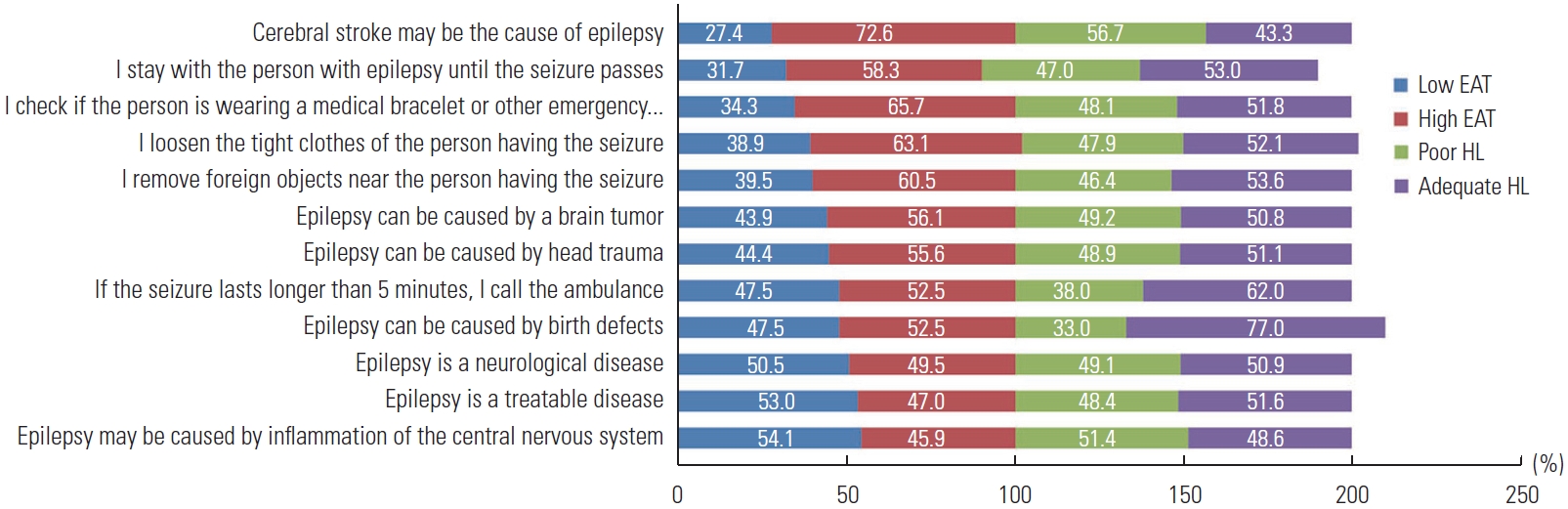
Relationship between items of EAW and scores for EAT and HL. EAW, epilepsy awareness; EAT, epilepsy attitudes; HL, health literacy.
DISCUSSION
The quality of life of school-age children and youth with epilepsy may be affected by negative attitudes in the school environment and poor awareness of the disease. This can increase the fragility of students with epilepsy. Teachers are leaders in supporting and ensuring the safety of students with epilepsy. However, their low awareness of the disease may leave teachers helpless about first-aid practices during their shifts.
In the literature, it has been demonstrated that teachers’ understanding of epilepsy differs according to country. Whereas teachers’ understanding of epilepsy was low in Turkey, Greece, Japan, and Kuwait [22-25], it was found to be moderate in Jordan [26] and high in Saudi Arabia [27].
The current study determined that participating teachers’ attitudes towards epilepsy were negative, their awareness was low, and their HL level was limited (Table 1). Other studies have reported that teachers’ awareness of the disease was low, their attitudes were negative, and their awareness of first-aid practices during a seizure was insufficient [28-31].
This study concurs with the literature that insufficient awareness about epilepsy leads to negative attitudes. On the other hand, teachers’ low awareness and negative attitudes towards the disease coincided with their HL limitations (Tables 2 and 3). The situation reflects teachers’ HL levels. In fact, it was observed that the most vital determinant of low awareness is limited HL (Table 3). Limited HL among teachers is a global problem that creates a barrier to disease awareness [32-35].
In the present study, female teachers were more aware of epilepsy and had more positive attitudes than male teachers (Table 1), and in an Iranian study, it was revealed that female teachers had greater knowledge of the disease [36]. This result may be due to the social structure and characteristics of the society. Female teachers may be more sensitive to the disease with the responsibilities brought by a maternal role.
In this study, it is a pleasing result that EAW was relatively high among primary school teachers. Indeed, epilepsy is the most common chronic neurological pathology in children, and 1 in every 150 children worldwide has epilepsy in the first 10 years of life [37]. Children and teens with epilepsy are at risk for seizures; teachers are the first to respond if a child has a seizure while at school. Teachers should know when to transfer patients to the hospital and should be able to provide first aid for seizures.
During a generalized seizure, the teacher’s role is to keep the student in a safe position and monitor the student for the duration of the seizure. Patients should be placed in the recovery position when the seizure is over. In this study, one of the influential factors on disease awareness was having an individual with epilepsy in the participant’s family/social environment or the classroom and having witnessed an epileptic seizure (Tables 2 and 3). Being near individuals with epilepsy and witnessing seizures can heighten awareness of the disease. Nonetheless, although large numbers of epileptic seizures are witnessed by teachers [38,39], it was also reported that the rate of receiving first-aid training was low [40].
This study, conducted in a city in the Central Black Sea region of Turkey, showed that teachers’ negative attitudes and limited HL levels indicated their limited awareness of epilepsy. Knowledge gaps regarding the cause of the disease, risk factors, and first aid practices may result from prejudices about the disease. Panels, workshops, and health training on epilepsy should be organized for school teachers and included in certified first aid practices at regular intervals. It is suggested that future research be conducted to evaluate teachers’ EAW, EAT, and skill tendencies in first-aid practice. In addition, teachers’ health competencies should be assessed.
SUPPLEMENTAL MATERIALS
Supplemental materials are available at https://doi.org/10.3961/jpmph.23.330.
Supplemental Material 1.
EPILEPSY AWARENESS SCALE
Supplemental Material 2.
EUROPEAN HEALTH LITERACY SCALE
Notes
CONFLICT OF INTEREST
The author has no conflicts of interest associated with the material presented in this paper.
FUNDING
None.
AUTHOR CONTRIBUTIONS
All work was done by GY.
ACKNOWLEDGEMENTS
None.