Effect Modification of Kidney Function on the Non-linear Association Between Serum Calcium Levels and Cardiovascular Mortality in Korean Adults
Article information

Abstract
Objectives
This study aimed to evaluate the potential interaction between kidney function and the non-linear association between serum calcium levels and cardiovascular disease (CVD) mortality.
Methods
This study included 8927 participants enrolled in the Dong-gu Study. Albumin-corrected calcium levels were used and categorized into 6 percentile categories: <2.5th, 2.5-25.0th, 25.0-50.0th, 50.0-75.0th, 75.0-97.5th, and >97.5th. Restricted cubic spline analysis was used to examine the non-linear association between calcium levels and CVD mortality. Cox proportional hazard regression was used to estimate hazard ratios (HRs) for CVD mortality according to serum calcium categories. All survival analyses were stratified by the estimated glomerular filtration rate.
Results
Over a follow-up period of 11.9±2.8 years, 1757 participants died, of whom 219 died from CVD. A U-shaped association between serum calcium and CVD mortality was found, and the association was more evident in the low kidney function group. Compared to the 25.0-50.0th percentile group for serum calcium levels, both low and high serum calcium tended to be associated with CVD mortality (<2.5th: HR, 6.23; 95% confidence interval [CI], 1.16 to 33.56; >97.5th: HR, 2.56; 95% CI, 0.76 to 8.66) in the low kidney function group. In the normal kidney function group, a similar association was found between serum calcium levels and CVD mortality (<2.5th: HR, 1.37; 95% CI, 0.58 to 3.27; >97.5th: HR, 1.65; 95% CI, 0.70 to 3.93).
Conclusions
We found a non-linear association between serum calcium levels and CVD mortality, suggesting that calcium dyshomeostasis may contribute to CVD mortality, and kidney function may modify the association.
INTRODUCTION
Serum calcium is a crucial component for skeletal mineralization and a critical factor for essential bodily functions, including the coagulation pathway, muscle contraction, and neurological function [1]. Calcium dysregulation has various adverse health effects. Hypercalcemia may be associated with pathological processes, including vascular calcification and hypercoagulation, whereas hypocalcemia can adversely affect cardiac conduction and lead to heart failure and arrhythmia [2].
Most previous studies have found serum calcium levels to be positively associated with cardiovascular events [3] and all-cause mortality across the general population [1,3]. However, some studies have found that low levels of serum calcium are also associated with mortality related to certain medical conditions, including myocardial infarction [4], coronavirus disease 2019 (COVID-19) [5], and trauma [6], while others found a U-shaped association among the Danish general population [7] and intensive care unit patients [8]. Some studies have also indicated a positive association between serum calcium levels and cardiovascular disease (CVD) events and CVD mortality. Despite these findings, there is still limited evidence regarding the association between serum calcium levels and CVD mortality, and the shape of this association has not been sufficiently investigated. Chronic kidney disease (CKD) alters mineral metabolism and can promote pathophysiological processes of calcium dyshomeostasis, including vascular calcification and arrhythmia [9,10]. Although various studies have linked both high and low serum calcium levels to mortality in patients with CKD [11-13], it remains unclear whether this association varies among individuals with and without CKD. Previous studies in Korea have primarily focused on the association between serum calcium levels and all-cause mortality among both the general population and those with specific medical conditions. However, no studies have investigated the association between serum calcium levels and CVD mortality.
This study aimed to investigate the non-linear association between serum calcium levels and CVD mortality among the Korean population. In addition, we examined various effect modifications on the association between serum calcium levels and CVD mortality according to kidney function.
METHODS
Study Population
This study included participants from the Dong-gu Study, which was conducted from 2007 to 2010 and investigated risk factors for chronic diseases among a prospective cohort from the general population aged 50 years and above and in Gwangju, Korea [14]. Of the 9260 participants, 32 individuals with missing values for serum calcium or serum albumin levels and 301 individuals with missing values for the covariates were excluded from the analyses. A total of 8927 participants who were followed up for a period of 11.86±2.82 years were included in the analysis.
Measurements
After overnight fasting, venous blood samples were obtained in the morning. Serum calcium levels and total cholesterol levels were measured using an automatic analyzer (Hitachi-7600; Hitachi, Tokyo, Japan). According to our laboratory reference range, the reference range for the total serum calcium level was 8.4-10.2 mg/dL (2.1-2.6 mmol/L). In our population, the range between the 2.5th percentile to the 97.5th percentile for the total serum calcium level was 8.4-10.2 mg/dL. Serum calcium is usually bound to albumin, and measured serum calcium levels may underestimate biologically active calcium levels. Therefore, measured calcium levels were corrected using Payne’s formula:
Corrected calcium level, mg/dL= total calcium level, mg/dL+0.8×[normal albumin level, 4 g/dL - patient’s albumin level, g/dL] [15]
Data on demographics, education status, lifestyle, and disease history were obtained through questionnaires. Age was categorized into 3 groups: under 60 years, 60-75 years, and 75 years or older [16]. Education level was categorized into 2 groups: 9 years or more of formal education and less than 9 years of formal education. Physical activity was defined as walking for at least 30 minutes per day and at least 5 times per week. Smoking status classifications were non-smoker, former smoker, and current smoker. Drinking status classifications included non-drinker, former drinker, and current drinker. Diabetes and hypertension were defined as those who took medications for diabetes and hypertension, respectively. Body mass index (BMI) was calculated using the participants’ measured heights and weights and categorized into 4 groups based on the World Health Organization classification system: <18.5 kg/m2 (underweight), 18.5-24.9 kg/m2 (normal), 25.0-29.9 kg/m2 (overweight), and >30.0 kg/m2 (obese). The 2012 CKD-Epidemiology Collaboration Creatinine-Cystatin C equation was used to calculate the estimated glomerular filtration rate (eGFR) [17], which was categorized into 2 groups: eGFR ≥60 mL/min/1.73 m2 (normal) and eGFR <60 mL/min/1.73 m2 (CKD stages 3-5).
Ascertainment of Death
Death was confirmed using death records from the National Statistical Office up to December 31, 2021. Data on dates and causes of death were confirmed using death records, and the causes of death were coded according to International Classification of Diseases 10th revision (ICD-10) codes. Death from CVD falls under the ICD-10 codes I20-I25 and I60-I69.
Statistical Analysis
Using the adjusted calcium levels, the participants were classified into 6 categories based on the following percentiles: <2.5th, 2.5-25.0th, 25.0-50.0th, 50.0-75.0th, 75.0-97.5th, and >97.5th. The baseline characteristics of the participants were presented as the mean±standard deviation or number (%). Based on the categorized calcium levels, the participants’ characteristics were compared using analysis of variance (ANOVA) for continuous variables and the chi-square test for categorical variables. In addition, baseline characteristics according to kidney function status were compared using the independent t-test and the chi-square test. A restricted cubic spline with 4 knots was used in the Cox proportional hazard model analyses to evaluate the non-linear associations between the corrected calcium levels, which were considered continuous variables, and all-cause and CVD mortality. Hazard ratios (HRs) for the corrected calcium levels were presented with reference calcium levels set at the lowest predicted risk for the outcome. The non-linearity of the restricted cubic spline models was tested by comparing the linear and non-linear models using ANOVA. The interaction between serum calcium levels and kidney function was tested by comparing the non-linear model with the interaction term and the non-linear model without the interaction term. In addition, restricted cubic spline models depicting the association between serum calcium and all-cause and CVD mortality were fitted according to age, sex, BMI, hypertension, and diabetes. The interaction between serum calcium levels and each covariate was evaluated. To evaluate the association between the categorized calcium levels and all-cause and CVD mortality, Cox proportional hazard regression analyses were performed after adjusting for age, sex, education level, physical activity, smoking status, drinking status, BMI, hypertension, diabetes, and total cholesterol. In the Cox proportional regression model, the serum calcium level-based category with the lowest risk was selected as the reference group. Covariates were selected based on previous studies [18-21]. Statistical significance was considered to be indicated by a p-value of <0.05. All analyses were performed using R version 4.2.2 (R Foundation for Statistical Computing, Vienna, Austria).
Ethics Statement
This study was approved by the Institutional Review Board of Chonnam National University Hospital (IRB No. I-2008-05-056). Informed consent was obtained from all participants when they were enrolled in the baseline examination.
RESULTS
The baseline characteristics of the participants according to their calcium levels are presented in Table 1. Of the 8927 participants, 1757 (19.7%) died during the study period, of which 219 died from CVD. Participants in the 2.5-25.0th percentile for calcium levels tended to be younger and included a higher proportion of female, participants with more than 9 years of education, current smokers, current drinkers, participants with a normal BMI, participants with diabetes, and participants with hypertension compared to the other percentile groups. Participants with higher calcium levels tended to have higher total cholesterol levels. The proportion of participants who died overall and those who died from CVD were lowest among the participants in the 2.5-25.0th and 25.0-50.0th percentile groups. Moreover, the follow-up duration was longer for participants with the lowest calcium levels than for participants in the other groups.

Baseline characteristics of the study population according to the serum calcium concentration-based categories
In Supplemental Material 1, the baseline characteristics of the study participants are presented according to kidney function. Specifically, of the 8927 total participants, 641 (7.2%) had impaired kidney function, with most at stage 3a (71.8%). The distribution of the eGFR was similar to that of a previous study of the Korean general population [22]. The impaired kidney function group had higher adjusted serum calcium levels, allcause mortality, and CVD mortality. Kidney function was associated with age, education level, lifestyle factors, BMI, and comorbidities.
Figure 1 shows the non-linear association between adjusted calcium levels and CVD mortality according to kidney function. In both the impaired kidney function group and the normal kidney function group, there was a U-shaped association between serum calcium levels and CVD mortality, with low points of 8.73 mg/dL (2.18 mmol/L) and 8.67 mg/dL (2.17 mmol/L), respectively. These associations were more evident in the kidney impairment group (p=0.043 for interaction), and the non-linearity of these associations was significant only in the kidney impairment group (eGFR<60 mL/min/1.73 m2=0.028; eGFR≥60 mL/min/1.73 m2=0.349).

HRs of cardiovascular mortality according to adjusted serum calcium levels and kidney function status. Ref, reference value; HR, hazard ratio; eGFR, estimated glomerular filtration rate. HR were estimated using the restricted cubic spline model of 4 knots adjusted for age, sex, education level, physical activity, smoking status, drinking status, body mass index, comorbidities (diabetes, hypertension), and total cholesterol. The rug plot represents the distribution of adjusted serum calcium levels.
Supplemental Material 2 depicts the non-linear association between the adjusted calcium levels and overall mortality according to kidney function. The association between serum calcium levels and overall mortality was U-shaped in the impaired kidney function group; however, the non-linearity in each kidney function group was not statistically significant (eGFR <60 mL/min/1.73 m2=0.288; eGFR ≥60 mL/min/1.73 m2=0.122).
Supplemental Material 3 depicts the non-linear association between adjusted calcium levels and overall and CVD mortality according to the covariates (age, sex, BMI, hypertension, diabetes). The non-linear association between serum calcium and overall mortality was significant in participants under 75 years of age, female, and those with a BMI under 25 kg/m2. The nonlinear association between serum calcium levels and CVD mortality was significant in participants under 75 years of age, male, those with a BMI under 25 kg/m2, and those without hypertension. However, the interaction on the association according to the covariates was not significant except with regard to age.
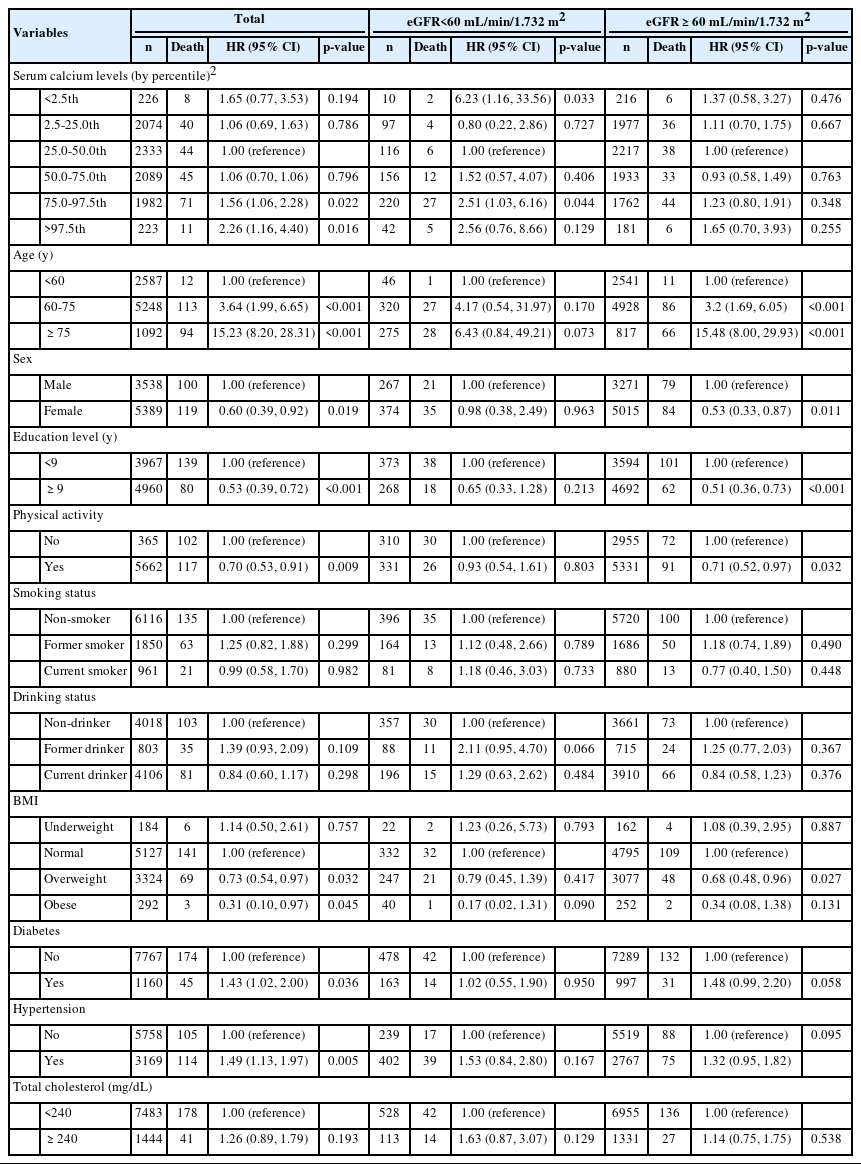
Table 2 shows the association between the adjusted calcium levels and CVD mortality according to kidney function. The results from various models indicated a U-shaped association between calcium levels and CVD mortality. This association was more pronounced in individuals with reduced kidney function, although the statistical analysis did not identify a significant interaction in the categorical analysis (p=0.370 for interaction). Among the total population, the HRs for CVD mortality in the 2.5th percentile or lower group and the 97.5th percentile or higher group were 1.65 (95% confidence interval [CI], 0.77 to 3.53) and 2.26 (95% CI, 1.16 to 4.40), respectively, compared to the 25.0-50.0th percentile group. In the impaired kidney function group, the HR for CVD mortality in the 2.5th percentile or lower group was 6.23 (95% CI, 1.16 to 33.56), and the HR for CVD mortality in the 97.5th percentile or higher group was 2.56 (95% CI, 0.76 to 8.66) compared to the 25.0-50.0th percentile group. In the normal kidney function group, the HRs for CVD mortality in the 2.5th percentile or lower group and the 97.5th percentile or higher group were 1.37 (95% CI, 0.58 to 3.27) and 1.65 (95% CI, 0.70 to 3.93), respectively, compared to the 25.0-50.0th percentile group.
Supplemental Material 4 shows the association between adjusted calcium levels and overall mortality according to kidney function. All models showed a U-shaped association between calcium levels and overall mortality, which tended to be stronger in groups with low kidney function, but the interaction was not statistically significant in this categorical analysis (p=0.610 for interaction).
DISCUSSION
In this study, we observed a U-shaped relationship between serum calcium levels and CVD mortality among the general Korean population. We found that the lowest risk of CVD mortality was associated with low-normal levels of serum calcium. This association was modified by kidney function, with a stronger effect observed in individuals with reduced kidney function.
A previous study investigating the association between serum calcium and CVD mortality across 2 general populations from the UK biobank and the US National Health and Nutrition Examination Survey found a U-shaped association in each cohort, showing similar results to those in our study [23]. However, there was limited evidence regarding the association between serum calcium levels and CVD mortality. Some studies of the general population have identified a non-linear association between serum calcium levels and mortality. In a study of 1 967 622 participants using data from the US Department of Veterans Affairs, serum calcium levels showed a U-shaped relationship with all-cause mortality; furthermore, a higher mortality rate was found among Black participants with low serum calcium levels than among White participants [24]. In a study of 20 512 subjects from the Copenhagen general practice sector, serum calcium levels showed a U-shaped association with all-cause mortality [7].
Previous studies have suggested that there are several pathways linking serum calcium levels to mortality, with most of the pathways involving the detrimental cardiovascular effects of high serum calcium levels. First, calcium regulates cell signaling, including cell proliferation and the electrochemical gradient of excitable cells, including neuronal axons. In addition, perturbed calcium homeostasis can cause pathologic responses in calcium-regulated mechanisms, such as oxidative stress and neuronal dysfunction. Indeed, calcium dyshomeostasis is associated with malignant disease [25], neurodegenerative disease [26], and the pathogenesis of obesity and diabetes [27]. Second, low or high serum calcium levels can disrupt neuromuscular stability. Abnormal serum calcium levels can affect cardiomyocytes and conductive system functioning, which can lead to heart failure, QT prolongation or shortening, and arrhythmias, including atrial fibrillation [28]. Third, elevated serum calcium concentrations alter the vascular microenvironment, thereby increasing intravascular plaque formation and mineral deposits [29].
Furthermore, the association between serum calcium levels and CVD mortality was more evident in the group with low kidney function than in the normal kidney function group. No previous study has evaluated whether serum calcium levels and mortality change according to kidney function. However, 3 previous studies examining CKD patients have all reported a U-shaped association between serum calcium levels and mortality. Among 107 200 patients on hemodialysis in the United States, the association between albumin-corrected serum calcium levels and mortality showed a U-shaped association, with low points of 8.5-10.0 mg/dL [11]. Hemodialysis patients in the Dialysis Outcomes and Practice Patterns Study cohort showed a similar association, with low points at 8.5-10.0 mg/dL [12]. In patients with CKD who do not need dialysis, the time-averaged serum calcium levels were found to have a U-shaped association with mortality, with the lowest risk being found among those with serum calcium levels of 9.0-9.5 mg/dL serum [13]. This finding may provide evidence for adverse health effects caused by high or low calcium levels that can be exacerbated by CKD. First, cardiac tissue is vulnerable to damage from conditions associated with CKD, which can lead to clinical conditions that are susceptible to arrhythmia through various pathways [9]. In addition, CKD patients are prone to ventricular arrhythmias, and cardiac arrhythmias are the leading cause of death in dialysis patients [30]. CKD can also cause or promote vascular calcification through disturbances in bone metabolism, inflammation, and the increased burden of advanced glycation end products [10].
The present analysis found a non-linear association between serum calcium concentration and mortality, with the lowest risk of CVD mortality observed among those with low-normal serum calcium levels. However, most previous studies reported that the full normal range of serum calcium levels was associated with the lowest risk of mortality [7,11-13,24]. A study comparing the association by race between serum calcium levels and overall mortality, coronary heart disease, and ischemic stroke found that the serum calcium levels with the lowest risk of coronary heart disease were lower in White participants than in Black participants. Specifically, low-normal levels of serum calcium (8.5-8.8 mg/dL; 2.13-2.20 mmol/L) were associated with the lowest risk of coronary heart disease in Black participants and ischemic stroke in both races. These results suggest that the serum calcium levels with the lowest risk of various negative health outcomes may differ by race. Therefore, the differences in serum calcium levels with the lowest risk in the present analysis may be attributed to differences in the study population and health outcomes. In addition, differences in measurements and analytic methods may have affected the results.
There are several limitations to this study that should be considered. First, the analysis was conducted using observational data; therefore, the results should not be used to construe a causal non-linear association between serum calcium levels and mortality. There may be unknown confounders associated with serum calcium levels and mortality. In the present study, chronic disease and its related biomarkers and lifestyle factors were adjusted. Second, the biologically active form of calcium—ionized serum calcium—was not measured; instead, albumin-corrected calcium levels were used in this analysis. Most biologically inactive calcium is albumin-bound, and albumin-corrected calcium levels usually reflect ionized serum calcium levels. Furthermore, the reproducibility of measuring ionized calcium is less reliable than measuring total calcium. Therefore, clinical guidelines recommend using adjusted calcium levels rather than ionized calcium levels for CKD patients [31,32].
In conclusion, the association between serum calcium levels and CVD mortality among the Korean general population is Ushaped, and the non-linear association may be modified by kidney function. These findings suggest that both elevated and decreased serum calcium levels may be involved in the pathogenesis of CVD and that the association can be modified by kidney function. The present study underscores the importance of maintaining optimal serum calcium levels to prevent adverse health outcomes, including CVD, and considering kidney function when evaluating the association between serum calcium levels and mortality in Korea. This comprehensive understanding could be used to improve preventive strategies and guide future research to further understand the complex interplay between serum calcium levels, kidney function, and cardiovascular health.
SUPPLEMENTARY MATERIALS
Supplemental materials are available at https://doi.org/10.3961/jpmph.23.068.
Notes
CONFLICT OF INTEREST
The authors have no conflicts of interest associated with the material presented in this paper.
FUNDING
None.
AUTHOR CONTRIBUTIONS
Conceptualization: Shin MH. Formal analysis: Yang JH, Shin MH. Funding acquisition: None. Methodology: Shin MH. Writing – original draft: Yang JH, Shin MH. Writing – review & editing: Yang JH, Kweon SS, Lee YH, Choi SW, Ryu SY, Nam HS, Kim HY, Shin MH.
ACKNOWLEDGEMENTS
None.