Prevalence of Sarcopenia Among the Elderly in Korea: A Meta-Analysis
Article information

Abstract
Objectives
Sarcopenia is a common disease in the elderly population that causes disability, poor quality of life, and a high risk of death. In the current study, we conducted a meta-analysis to report basic knowledge about the prevalence of sarcopenia in the elderly in Korea.
Methods
We searched for articles in the MEDLINE, Cochrane Library, Embase, and Scopus databases published until December 28, 2020. Studies investigating the prevalence of sarcopenia in elderly Koreans aged ≥65 years were included. The methodological quality of the studies was evaluated using the Newcastle-Ottawa scale. Publication bias was evaluated using the Egger test and funnel plots.
Results
In total, 3 studies and 2922 patients were included in the meta-analysis. All 3 studies used the European Working Group on Sarcopenia in Older People criteria for the diagnosis of sarcopenia. The total prevalence of sarcopenia was 13.1-14.9% in elderly men and 11.4% in elderly women.
Conclusions
This meta-analysis is the first to estimate the pooled prevalence of sarcopenia in elderly Koreans, and its findings suggest that sarcopenia is common in this population. Therefore, attention should be paid to the prevention and control of sarcopenia.
INTRODUCTION
Sarcopenia refers to a condition wherein the body’s muscle mass and strength are abnormally decreased or weakened [1]. It is an age-related disease. In general, 1-2% of muscle is lost every year starting at the age of 50 years [2]. In older people, sarcopenia is a major problem that causes disability, poor quality of life, and a high risk of death [3]. In Korea, the prevalence of sarcopenia is increasing because of the increase in the elderly population and life expectancy [4].
As clinicians’ and researchers’ interest in sarcopenia has increased, several studies have investigated its prevalence [5-7]. However, the prevalence of sarcopenia has been inconsistent in different studies, and no large-scale epidemiological study of sarcopenia has yet been carried out in Korea.
In the current study, we conducted a meta-analysis and systematically evaluated the prevalence of sarcopenia in elderly Koreans to construct basic data on the prevalence of sarcopenia in Korea.
METHODS
Search Strategy
This meta-analysis was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) guidelines [8]. We systematically searched for relevant articles in the PubMed, Embase, Cochrane Library, and Scopus databases for studies published up to December 28, 2020. The following keywords were used in the search: (sarcopenia OR muscle mass OR muscle strength) AND (prevalence OR epidemiology OR frequency OR incidence) AND (Korea).
Study Selection
We applied the following inclusion criteria for the selection of articles: (1) the prevalence rate of sarcopenia was evaluated, (2) the study was conducted among Koreans, (3) age of the included subjects was ≥65 years, and (4) loss of appendicular muscle mass and functional decline were considered for the diagnosis of sarcopenia. The exclusion criteria were (1) the same data published repeatedly, and (2) not reporting study outcomes.
Data Extraction
After discarding duplicate studies, 2 reviewers (YJC and MCC) independently evaluated the potentially eligible studies. The articles were screened for eligibility by reviewing the title and abstract. Disagreements were resolved through consensus. After screening, the full texts of the eligible articles were read independently by both reviewers, and the eligibility of each article was re-assessed. Subsequently, data on the first author, publication date, study type, number of patients, and demographic characteristics (age, gender, and other participant details) were extracted.
Quality Assessment
The Newcastle-Ottawa scale (NOS) for cross-sectional studies was used for quality assessment [9], with 3 aspects (selection, comparability, and outcomes). The judgment of bias was expressed as “unsatisfactory,” “satisfactory,” “good,” or “very good.” The quality of each study was graded as unsatisfactory (0-4), satisfactory (5-6), good (7-8), or very good (9-10). All differences of opinion were resolved by consensus.
Statistical Analysis
Using the Comprehensive Meta-Analysis version 2 (Biostat Inc., Englewood, NJ, USA), the extracted data were analyzed using statistical tests. For each analysis, a heterogeneity test was conducted using the I2 statistic to evaluate the extent of inconsistency in the obtained results. If the I2 value was >50%, the data were considered to have substantial heterogeneity, and a random-effects model was used for data analysis. In contrast, if the I2 value was ≤50%, then the pooled data were considered homogeneous and a fixed-effects model was applied for data analysis. The pooled prevalence and 95% confidence interval (CI) of sarcopenia were also calculated.
Ethics Statement
Ethical approval was waived because this was a meta-analysis based on previously published studies.
RESULTS
Study Selection
In total, 721 potentially relevant studies were selected in the preliminary search of all the databases (Figure 1). We excluded 224 duplicate studies and excluded an additional 481 publications after their titles and abstracts were reviewed. The remaining studies were assessed through a review of the full texts of the articles. As a result of full-text screening, 3 articles were included (Table 1) [10-12]. In all 3 articles, the European Working Group on Sarcopenia in Older People (EWGSOP) criteria [13] were used for the diagnosis of sarcopenia.

Flow chart showing the search results of the metaanalysis.

Characteristics of the included studies
Study Characteristics
The selected studies included 2922 patients (male-to-female ratio, 1455:1467). The characteristics of the selected studies are summarized in Table 1.
Risk of Bias
All the included studies were rated 5 points (selection: 2 points; outcome: 3 points). Therefore, the quality of the 3 studies assessed using the NOS was considered satisfactory.
Meta-analysis Results
To analyze the prevalence, a random-effects model was used (I2 for total prevalence among elderly people, 97.1%; for prevalence among elderly men, 95.8%; and for prevalence among elderly women, 90.4%). The total prevalence of sarcopenia among elderly Koreans aged ≥65 years was 13.1% (95% CI, 6.1 to 25.9) (Figure 2). The prevalence of sarcopenia among elderly Korean men was 14.9% (95% CI, 6.3 to 31.5), whereas the prevalence of sarcopenia among elderly Korean women was 11.4% (95% CI, 6.1 to 20.5).
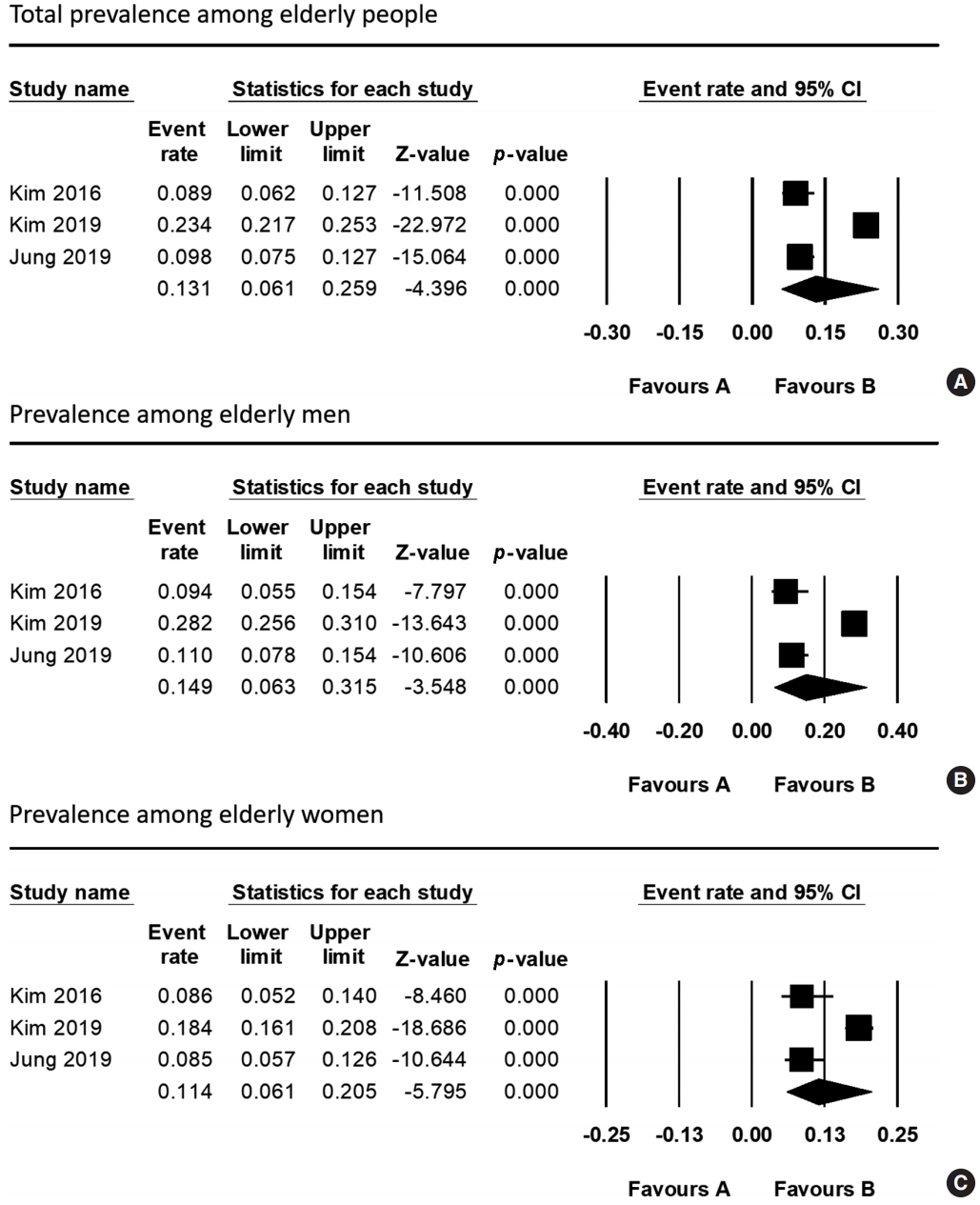
Results of the meta-analysis of sarcopenia prevalence (A: total, B: men, C: women). CI, confidence interval.
Publication Bias
Funnel plot analysis and the Egger test were performed. Funnel-plot analyses revealed symmetrical results (Figure 3). In addition, all p-values for the Egger test were >0.05 (total prevalence among elderly people: p=0.301; prevalence among elderly men: p=0.069; prevalence among elderly women: p=0.059). Therefore, publication bias was not significant.
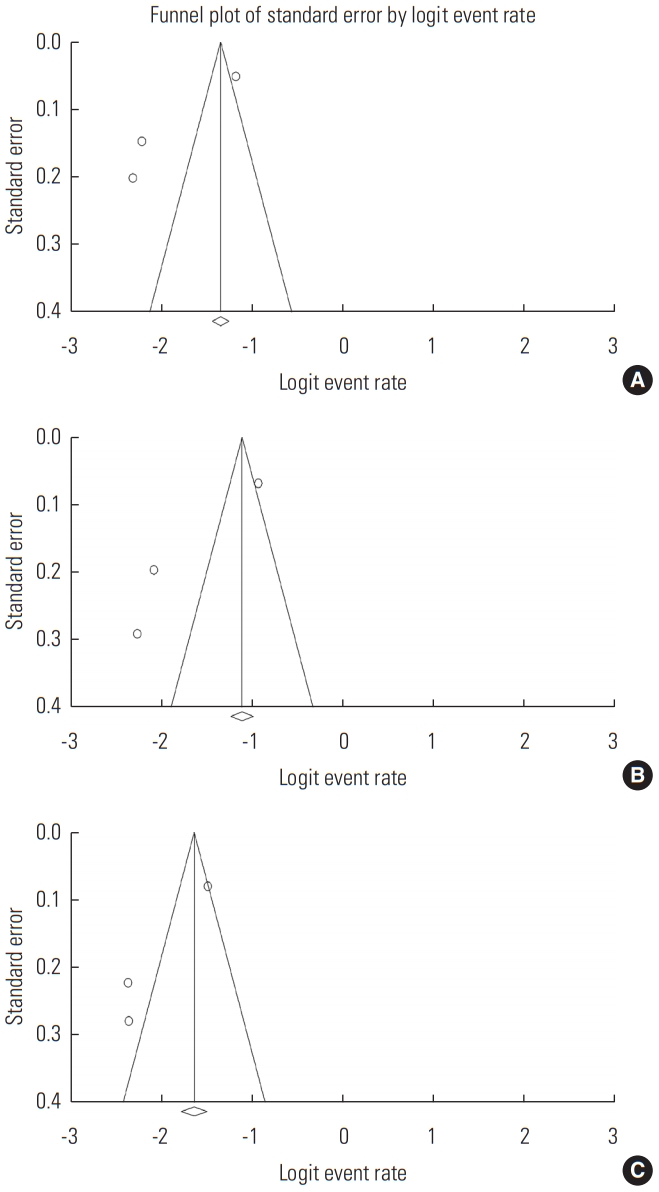
Funnel plots of the included studies (A: total, B: men, C: women).
DISCUSSION
A meta-analysis was performed to determine the prevalence of sarcopenia in the elderly Korean population. The results showed that the overall prevalence was 13.1%; the prevalence in men was 14.9% and that in women was 11.4%. All 3 included studies used the EWGSOP criteria for the diagnosis of sarcopenia.
Although the results of previous studies on the prevalence of sarcopenia are heterogeneous, generally it has been reported to range from 10% to 20% [14-17]. Our results are similar to those of previous studies. In addition, in our study, men showed a higher prevalence of sarcopenia than women, which is consistent with the results of several previous studies [2,18- 20]. Some possible reasons for this have been suggested. First, the prevalence of sarcopenia increases in patients with diabetes, and since men generally have a higher prevalence of diabetes than women, the prevalence of sarcopenia in men may therefore be higher [21]. Second, a higher prevalence of sarcopenia in men could be related to their higher smoking rate, especially in men in Korea [5,22]. Since smoking decreases the amount of blood flow, the amount of oxygen provided to the muscles is reduced. In addition, smoking interferes with normal breathing, and consequently, gas exchange in the lungs cannot be performed normally, which makes it difficult for the muscles to receive oxygen [23]. When muscles are not properly supplied with oxygen, muscle growth is inhibited, which causes sarcopenia. Third, higher alcohol consumption in Korean men could result in a higher prevalence of sarcopenia in men [14,24]. It has been reported that alcohol reduces the synthesis of proteins [25]. Since protein synthesis in muscles is an essential factor for muscle growth, excessive alcohol consumption increases the probability of developing sarcopenia [26]. Thus, stopping or reducing smoking and alcohol consumption in the elderly population would be helpful for preventing and treating sarcopenia. Furthermore, at least 2-4 sessions of combined aerobic exercise and resistance training every week and appropriate protein intake (at least 1 g/kg) are essential for the prevention and treatment of sarcopenia [27].
Regarding the prevalence of sarcopenia in other countries, Du et al. [28] surveyed 2458 elderly individuals (≥65 years of age) in the United States and reported that the total prevalence of sarcopenia was 15.51%. Lera et al. [29] reported that the prevalence of sarcopenia in 1006 elderly individuals (≥60 years of age) in Santiago, Chile was 19.1%. Liu et al. [30] investigated the prevalence of sarcopenia in 4500 elderly individuals (>60 years of age) in Yunnan, Guizhou, Sichuan, and Xinjiang in China and found it to be 19.3%. Generally, the prevalence of sarcopenia in Korea is lower than that in other countries. A variety of factors, such as differences in eating habits, the surrounding environment, culture, and race-specific genetics, may be responsible for differences in the prevalence of sarcopenia among countries [31-33].
To date, over a dozen studies have attempted to examine the prevalence of sarcopenia in Korea. However, the 3 studies included in our meta-analysis were the only ones that measured muscle function for the diagnosis of sarcopenia, instead of only considering appendicular muscle mass. Sarcopenia is defined as a condition characterized by loss of both skeletal muscle mass and function. Muscle strength depends on muscle mass, and the relationship between muscle strength and muscle mass is not linear [13]. Therefore, for the diagnosis of sarcopenia, both muscle mass and muscle function must be measured.
CONCLUSION
We found that the overall prevalence of sarcopenia in the elderly Korean population was 13.1%. The prevalence of sarcopenia in elderly men and women was 14.9% and 11.4%, respectively. This is the first study to systematically evaluate the prevalence of sarcopenia in Korea through a meta-analysis. However, our study is limited by the inclusion of a small number of studies and population. For more robust results, further well-designed studies with larger populations should be conducted in the future.
Notes
CONFLICT OF INTEREST
The authors have no conflicts of interest associated with the material presented in this paper.
FUNDING
The present study was supported by a National Research Foundation of Korea grant funded by the Korean government (grant No. NRF-2019M3E5D1A02068106).
ACKNOWLEDGEMENTS
None.
Notes
AUTHOR CONTRIBUTIONS
Conceptualization: YJC, MCC. Data curation: YJC, MCC. Formal analysis: YJC, MCC. Funding acquisition: MCC. Methodology: YJC, MCC. Visualization: YJC, MCC. Writing – original draft: YJC, MCC. Writing – review & editing: YJC, MCC.