Effects of the Out-of-pocket Payment Exemption in the Public Health Center on Medical Utilization of the Korean Elderly
Article information

Abstract
Objectives
The distribution of hospitals in Korea is unbalanced in terms of accessibility. Many local public health centers (PHCs) exempt out-of-pocket payments (OOPs) based on local government laws to increase coverage. However, this varies across administrative regions, as many make this exemption for the elderly, while others do not. This study aimed to evaluate the effects of the OOP exemption at local PHCs among elderly individuals.
Methods
This study used online data on Korean national law to gather information on individual local governments’ regulations regarding OOP exemptions. Individual-level data were gathered from the 2018 Community Health Survey and regional-level data from public online sources.
Results
The study analyzed 132 regions and 44 918 elderly people. A statistical analysis of rate differences and 2-level multiple logistic regression were carried out. The rate difference according to whether elderly individuals resided in areas with the OOP exemption was 1.97%p (95% confidence interval [CI], 1.07 to 2.88) for PHC utilization, 1.37%p (95% CI, 0.67 to 2.08) for hypertension treatment, and 2.19%p (95% CI, 0.63 to 3.74) for diabetes treatment. The regression analysis showed that OOP exemption had an effect on hypertension treatment, with a fixed-effect odds ratio of 1.25 (95% CI, 1.05 to 1.48).
Conclusions
The OOP exemption at PHCs can affect medical utilization in Korea, especially for hypertension treatment. The OOP exemption should be expanded to improve healthcare utilization in Korea.
INTRODUCTION
The function of public health centers (PHCs) in Korea, known as bogeonso, varies depending on the regional administrative division, population density, demographic distribution, and regional context. Unlike regions near Seoul, metropolitan areas, and large cities, PHCs play an important role in primary care in regions with a low population density and a small number of private hospitals. With the recent growth of the elderly population, many local governments have exempted out-of-pocket payments (OOPs), also known as a copayments, for the elderly at PHCs through local administrative laws. However, these laws vary from region to region, and there are still many places without the OOP exemption. Evidence of the effects of copayments has been obtained from earlier international studies [1], but in Korea’s regional context, with consideration of the magnitude of OOPs and national insurance coverage, the effects of these copayments may be of crucial importance when making public health policy.
After the enactment of the Regional Public Health Act in 1995, each local government has established a local healthcare plan every 4 years and revised related regulations based on these plans. Policy determinants include the number of people in the region, the finances and size of the local council, the characteristics of the head of local government, the voter turnout, and the social welfare budget [2]. After this act was enacted, several local governments implemented policies to reduce the copayments of the elderly at PHCs to meet the demands of the residents, and these policies seem to have spread through the policy diffusion effect [3-5].
The cost of OOPs at PHCs is not high in absolute terms, but many systematic reviews have nonetheless shown that increases in OOPs are associated with decreasing medical utilization and worse health outcomes, both in high-income and low-income countries [6,7].
The utilization of PHCs is positively associated with old age, female sex, low education and income levels, hypertension (HTN), and receiving Basic Livelihood Security Program benefits. PHC utilization is also associated positively with regions that have a high elderly population, a low number of healthcare workers per population, and low financial independence of the local government [8].
No studies have yet summarized the OOP exemption policies provided by local governments or analyzed their associations with medical utilization and health outcomes. Therefore, this study was conducted to evaluate the associations of OOP exemption policies at the municipality level with the utilization of PHCs and the treatment rate of chronic diseases such as HTN and diabetes mellitus (DM).
METHODS
Research Question
The PICO format was used to formulate the research question. The population (P) comprised elderly individuals living in local areas where PHCs are the main source of primary care. The intervention (I) was the local government policy of OOP exemption. The comparison (C) was elderly individuals living in local areas with no OOP exemption. The outcome (O) was utilization of PHCs and the treatment rate of HTN and DM. The research model is shown in Figure 1.
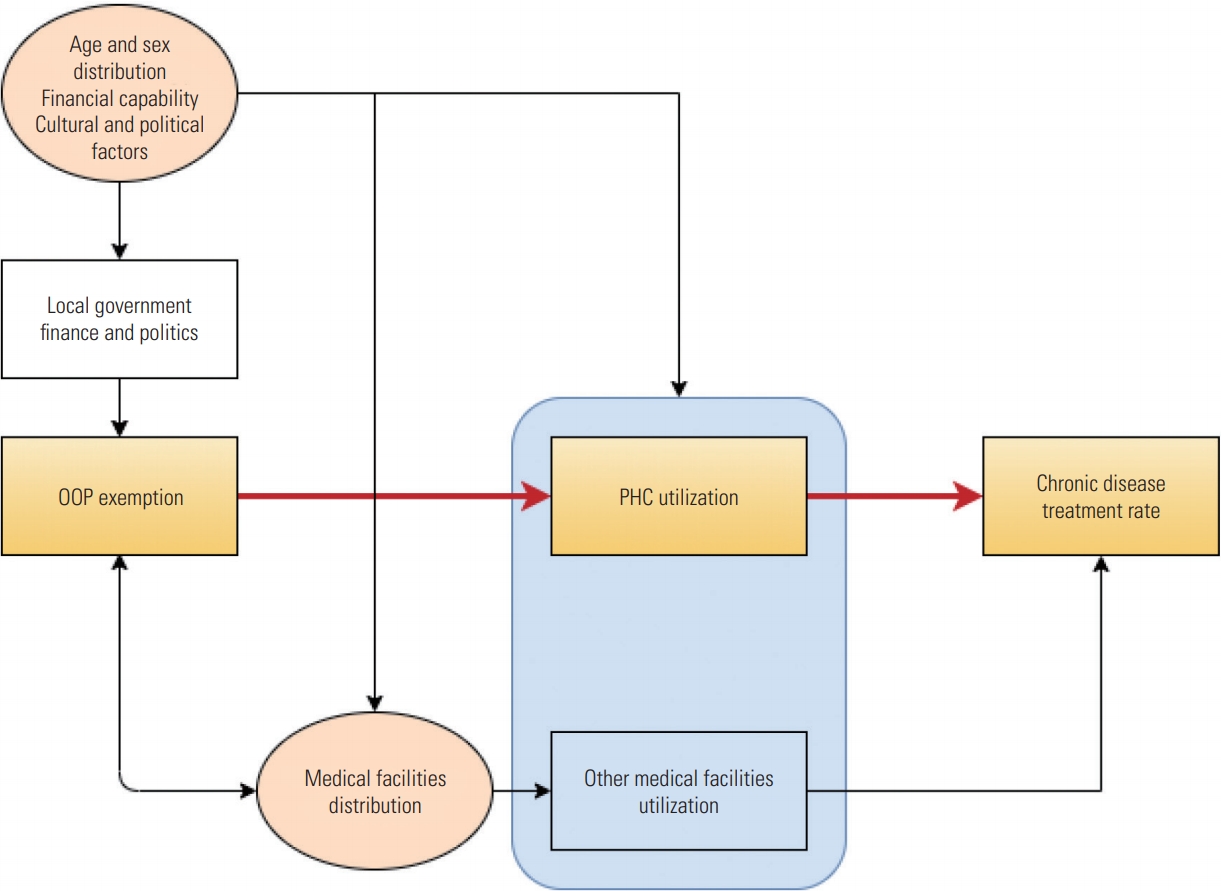
Causal model between out-of-pocket payment (OOP) exemption, public health center (PHC) utilization, treatment rate, and other variables to be considered.
Potential confounding factors were chosen using the causal theory of directional acyclic graphs [9], and included demographic factors, economic measures, and distribution of medical institutions.
Data Resources and Variables
Data on OOP exemption policies were gathered from the Korea Ministry of Government Legislation website (with the exclusion of Seoul, Sejong, and 6 metropolitan cities [gwangyeoksi]). Individual data were obtained from the 2018 Community Health Survey, which was conducted by the Korea Centers for Disease Control and Prevention among 228 340 respondents. Data on regional-level confounders were gathered from the Korean Statistical Information Service (http://kosis.kr/) and the Public Data Portal (https://www.data.go.kr/).
In total, 44 918 survey respondents were analyzed. The inclusion criteria were being 65 years of age or older, and the exclusion criteria were receiving Basic Livelihood Security Program benefits, residing in metropolitan cities, and residing in regions with at least 30 times more other medical facilities than PHCs; the final criterion was chosen to exclude regions where PHCs play a minimal role in providing primary care.
The dependent variable of medical utilization was analyzed based on the survey question asking whether the respondent had used a PHC in the last ear. HTN treatment was considered adequate if the patient took HTN medication more than 20 days in a month. DM treatment was considered adequate if the patient was taking medication or using insulin.
The main independent variable was OOP exemption at PHCs by local governmental laws, which differ across municipalities. Exemptions not relevant to medical utilization such as free vaccination programs were not included as OOP exemptions. The main focus was on distinguishing whether a person using a PHC for medical treatment needs to pay or not.
The other independent variables were the proportion of the elderly population, the number of PHCs (including health centers, headquarter of public health of the region; health center branches, facilities mainly of community medical care with 1 or 2 doctors; and healthcare centers, facilities mainly of chronic disease management without any doctors), the ratio of other medical facilities to PHCs at the region level, and sex, age, and household income at the individual level.
Statistical Analysis
This study used SAS version 9.4 (SAS Institute Inc., Cary, NC, USA) for the statistical analysis. A descriptive analysis was performed and rate differences in outcomes were calculated. Multilevel logistic regression was performed to evaluate the effects of independent variables.
The regression equation of the multilevel analysis in this study is as follows:
Yij: individual i in area j
Yij=1 : utilization of PHC / adequate treatment (HTN, DM)
β0j: mean log-odds of region j
Xij: j individual-level variables for region i (sex, age, household income)
β1j: slope of X1ij
γ00: intercept for β0j
Wj: j regional-level variables (OOP exemption, elderly population ratio, number of PHCs, ratio of other medical institutions)
γ01: slope of Wj reaching β0j prediction
u0j: error term for β0j in region j
γ10: intercept for β1j
γ11: slope of Wj reaching β1j prediction
This model involves 2-level multiple logistic regression analysis with a binary outcome. The model of this regression ignores the random slope effect since it is not logical to assume that individual-level variables would have different effects depending on the region. Instead, this model only assumes the random intercept effect. The final formula of the multilevel logistic regression was as follows:
The analysis consisted of 3 models. Model 1 was an empty model that only evaluated regional effects:
The intraclass correlation coefficient (ICC) was calculated.
Model 2 was an regression analysis with regional-level variables:
From the above equation, it was possible to investigate the degree to which the regional variables described the log-odds when individual variables were not considered.
Model 3 added individual-level variables, with the same equation as the overall regression equation presented above.
Ethics Statement
This study was approved by the Institutional Review Board (IRB) of Seoul National University (IRB No. E2004/002-003).
RESULTS
Descriptive Analysis
The current status of OOP exemption policies for the elderly in regions other than metropolitan cities in Korea is shown in Figure 2. Most of these regions have implemented these policies for more than 10 years, since the early 2000s.

Out-of-pocket payment (OOP) exemption.
In Gyeonggi Province, 30 regions had exemptions and 1 region did not. In Gangwon Province, 8 regions had exemptions and 10 regions did not. In North Chungcheong Province (11 regions) and Jeju Province (2 regions), all regions had exemptions. In South Chungcheong Province, 12 regions had exemptions and 2 regions did not. In North Jeolla Province, 6 regions had exemptions and 8 regions did not. In South Jeolla Province, 9 regions had exemptions and 13 regions did not. In North Gyeongsang Province, 9 regions had exemptions and 14 regions did not. In South Gyeongsang Province, 14 regions had exemptions and 4 regions did not.
The ratio of other medical facilities to PHCs was calculated by dividing the number of other medical facilities, such as private hospitals, by the number of medical PHCs (PHCs with medical care function, where they have medical doctors, including health centers and health center branches). Figure 3 shows a map of these ratios. Most of the regions with high ratios (>30) were adjacent to or near metropolitan areas, and they comprised 19 cities (si) and 2 districts (gu) in Gyeonggi Province, 5 cities and 7 districts in other regions, and no county (gun) regions.

Odds of other medical facilities to medical public health centers.
A descriptive analysis of the respondents to the Community Health Survey is shown in Table 1.

Descriptive analysis of the participants
There were, in total, 44 918 respondents, of whom 59.2% were females. The age distribution (in terms of 5-year intervals) was fairly even. The monthly household income was 500 000 Korean won (KRW) or less for 15.4% of participants, 500 000 KRW to 1 000 000 KRW for 31.6%, 1 000 000 KRW to 2 000 000 KRW for 27.6%, 2 000 000 KRW to 3 000 000 KRW for 12.0%, and more than 3 000 000 KRW for 13.4%.
The PHC utilization rate was 71.1%, and adequate treatment rates of HTN and DM were 91.2% and 83.4%, respectively.
Rate Differences
The weighted rate difference was calculated to compare the crude rates of the dependent variables between regions with OOP exemptions and the comparison regions without OOP exemptions (Table 2). In the OOP exemption regions, the PHC utilization rate was 62.0%, while it was 60.0% in the comparison regions, reflecting a statistically significant rate difference of 1.97%p (95% CI, 1.07 to 2.08), which means that regions with OOP exemptions had a PHC utilization rate that was 1.97%p higher than the comparison regions.

Rate difference and regression analysis
The treatment rate of HTN in the OOP exemption regions and the comparison regions was 91.8% and 90.5% respectively. The rate difference was 1.37%p (95% CI, 0.67 to 2.08), which was statistically significant; thus, regions with OOP exemptions had 1.37%p higher rates of adequate HTN treatment than the comparison regions.
The treatment rate of DM in the OOP exemption regions and the comparison regions was 84.4% and 82.2%, respectively. The rate difference was 2.19%p (95% CI, 0.63 to 3.74), and was statistically significant, meaning that regions with OOP exemptions had 2.19%p higher rates of adequate DM treatment than the comparison regions.
Logistic Regression
The results of the multilevel logistic regression analysis are shown in Table 2.
For PHC utilization, the ICC was calculated to be 0.146, meaning that regional differences explained 14.6% of PHC utilization. In model 2, among region-level independent variables, the proportion of the elderly population, the number of PHCs, and the ratio of other medical facilities showed statistical significance, as well as in model 3. The individual-level independent variables all showed statistical significance. The OOP exemption showed no effect on PHC utilization, while a proportionally larger elderly population, a lower number of PHCs, and a lower ratio of other medical facilities had a positive effect on the utilization of PHCs. Female sex, older age, and lower household income were also associated with higher PHC utilization.
For the treatment of HTN, the ICC was 0.049, meaning that 4.9% of variation in the treatment rate was explained by regional differences. Only the OOP exemption had a statistically significant effect on the HTN treatment rate at the regional level in model 2, as well as in model 3. The odds ratio was 1.21 (95% CI, 1.02 to 1.43) in model 2 and 1.25 (95% CI, 1.05 to 1.48) in model 3. The individual-level variables of age and household income showed statistical significance. Regions with the OOP exemption, a younger population, and a higher household income had higher rates of appropriate HTN treatment.
For DM treatment, the ICC was 0.046, meaning that regional differences explained 4.6% of the DM treatment rate. In model 2, among the region-level independent variables, the proportion of the elderly population and the ratio of other medical facilities showed statistical significance, as well as in model 3. As individual-level independent variables, age and household income showed statistical significance. Regions with a lower proportion of the elderly population, a lower ratio of other medical facilities, and individuals with a higher age and a generally higher household income showed higher rates of appropriate DM treatment.
DISCUSSION
This study summarized OOP exemption policies for the elderly across non-metropolitan regions in Korea for the first time, and showed that the lack of such a policy can hinder HTN treatment. Additionally, the effects of the relatively small amount of OOPs were analyzed quantitatively from the perspective of medical utilization.
Without adjustment, PHC utilization, HTN treatment, and DM treatment showed significant rate differences between regions with OOP exemption policies and those without OOP exemption policies. The multilevel logistic regression found that the presence of an exemption policy only had a significant effect on HTN treatment. Other regional factors, such as the number of PHCs, the ratio of other medical facilities, and the proportion of the elderly population, showed some effects on the outcomes, and individual factors such as sex, age, and household income showed some effects as well.
The geographical distribution of OOP exemption policies was found to be relatively homogeneous in Gyeonggi Province, South Chungcheong Province, North Chungcheong Province, and Jeju Province. Policy diffusion, demographic factors, and the distribution of medical facilities may have affected the spatial correlation of these policies. In the Korean context, the presence of high elderly population and rural areas in a region can affect the tax income of the local government, which may have affected the likelihood of implementing an exemption policy to reduce medical expenditures.
OOPs are defined as direct payments made by individuals to healthcare providers at the time of service use [10]. In Anderson’s healthcare utilization model, OOPs are a factor associated with individuals’ access to medical services [11,12]. However, it should be kept in mind that there are many non-financial factors that may also have affected medical utilization.
Nonetheless, several previous studies have found an association between high OOPs and reduced medical utilization [6,13,14]. Studies of OOPs in the Korean healthcare system also showed similar findings [15,16]. According to a recent study from the World Health Organization, OOPs (or copayments) may account for a large proportion of health financing, especially in countries with low public spending on health, but are not an effective rationing instrument due to strong and consistent evidence that they reduce necessary and unnecessary use in equal measure [17]. Regarding the treatment of chronic diseases, a systematic review showed that higher patient shares of medication costs were significantly associated with lower adherence [18], which implies that the treatment rate is associated with OOPs. The results of this study, therefore, showed partial concordance with previous studies.
Regarding PHC utilization, the rate difference was 1.97%p, whereas the regression analysis did not show a significant effect. One possible reason could be due to the questionnaire used to measure PHC utilization, which included any form of utilization of a PHC in the recent 1 year. PHCs provide free vaccinations and other free services, such as physiotherapy, acupuncture for smoking cessation, sports programs, dementia screening, and medical visits depending on the community and the local governments. The outcome of PHC utilization included all of these services; as such, it was not a fully representative outcome variable of medical utilization only.
The HTN and DM treatment rates were both higher in regions with the OOP exemption (rate difference, 1.37%p and 2.19%p respectively). In the logistic regression analysis, however, only HTN treatment showed a statistically significant effect from OOP exemptions. Unlike PHC utilization, the variables of HTN and DM treatment may reflect medical utilization more closely. However, the OOP exemption only had a statistically significant effect on HTN treatment. There could be many reasons why the effect on DM treatment was insignificant. A possible reason may be the different traits of DM and HTN treatment. Compared to HTN, DM treatment requires more invasive methods for follow-up, and indicators such as blood sugar levels fluctuate widely depending on dietary habits, physical status, and environmental factors. Insulin injections may also be needed, which are invasive and more complicated than taking drugs. These factors may explain why the treatment rate for DM was lower than the HTN treatment rate.
The limitations of this study are as follows.
Firstly, the data were limited to 2018, making this a cross-sectional study. Reverse causality is always possible, even though this policy has been implemented for a fairly long time.
Secondly, there is an issue regarding comparability (or exchangeability). The subjects from regions with and without OOP exemption policies should have homogeneous traits except for the variables of our interest, but it is difficult to ensure that the subjects had similar access to PHCs, political ideas, and cultural characteristics, since the subjects were not randomized.
Thirdly, not all expenditures for medical utilization were considered. Depending on where the elderly live, there may be variations in coverage. For instance, PHCs may offer drugs free of charge in some regions due to a lack of pharmacies, while that may not be the case in other regions. The local laws themselves are not binary and differences exist in the items that are covered. Additionally, some regions have financial support programs, such as the Hypertension/Diabetes Registration Management Program by the Korean Centers for Disease Control and Prevention, which was not considered in the analysis. Previous studies have also shown that even OOPs are covered, patients had to incur substantial costs to use free services in addition to travel costs [19].
Lastly, PHC utilization has limitations as a measure of medical utilization of PHCs due to the questionnaire-related problem stated above.
Despite its limitations, this study has reliability since it analyzed data from a large sample population. It should be noted that OOP exemptions had positive effects on HTN treatment, which supports further initiatives to expand the OOP exemption policy, even though the OOPs are relatively small when using PHCs. Through redistribution of wealth and improvements in coverage and accessibility, expanding the OOP exemption policy may have positive effects on health outcomes by improving the adequacy of HTN treatment, especially for elderly individuals in rural areas.
Notes
CONFLICT OF INTEREST
The authors have no conflicts of interest associated with the material presented in this paper.
FUNDING
None.
ACKNOWLEDGEMENTS
This paper is based on “Effects of out-of-pocket payment exemption in local public health center among Korean elderly in association with medical utilization and unmet medical need,” the lead author’s master’s thesis at the Graduate School of Public Health, Seoul National University.
Notes
AUTHOR CONTRIBUTIONS
Conceptualization: KN. Data curation: KN. Formal analysis: KN, EP. Funding acquisition: None. Methodology: KN, EP, CYK. Writing – original draft: KN. Writing – review & editing: KN, EP, YC, CYK.