Research Trends in Agenda-setting for Climate Change Adaptation Policy in the Public Health Sector in Korea
Article information

Abstract
Many studies have been conducted to assess the health effects of climate change in Korea. However, there has been a lack of consideration regarding how the results of these studies can be applied to relevant policies. The current study aims to examine research trends at the agenda-setting stage and to review future ways in which health-related adaptation to climate change can be addressed within national public health policy. A systematic review of previous studies of the health effects of climate change in Korea was conducted. Many studies have evaluated the effect of ambient temperature on health. A large number of studies have examined the effects on deaths and cardio-cerebrovascular diseases, but a limitation of these studies is that it is difficult to apply their findings to climate change adaptation policy in the health sector. Many infectious disease studies were also identified, but these mainly focused on malaria. Regarding climate change-related factors other than ambient temperature, studies of the health effects of these factors (with the exception of air pollution) are limited. In Korea, it can be concluded that studies conducted as part of the agenda-setting stage are insufficient, both because studies on the health effects of climate change have not ventured beyond defining the problem and because health adaptation to climate change has not been set as an important agenda item. In the future, the sharing and development of relevant databases is necessary. In addition, the priority of agenda items should be determined as part of a government initiative.
INTRODUCTION
Climate change can affect human health in 3 ways. First, it can directly affect human health through changes in the frequency of extreme weather events, such as heat waves, droughts, and heavy rain. Second, some effects of climate change on health are indirectly mediated by changes in the ecological system. Vectors of infectious diseases and air pollution exemplify mediating factors between climate change and human health. Lastly, climate change may disrupt human social or economic systems and subsequently influence food security or mental stress, which can impact human health down the line [1].
Recently, the World Health Organization (WHO) announced 10 challenges that pose a threat to human health, and climate change and air pollution were included along with non-communicable diseases such as diabetes and cancer, the global influenza pandemic, antimicrobial resistance, and vaccine hesitancy. In particular, the WHO considered climate change that causes premature death and disease to be a serious threat. Major air pollutants are expected to not only play a role in climate change, but also to increase morbidity and mortality [2].
In Korea, climate change-related health effects are becoming serious problems. During the summer season spanning from June 1 to August 16, 2018, the heat wave duration was 29.2 days, which was longer than in any other previous year (average, 8.7 days in other years) since 1973, when these statistics began to be recorded. The duration of tropical nights was 15.7 days (average, 4.4 days in other years), which was close to that of 1994 (16.6 days), which was recorded as the worst year for tropical nights [3]. According to a report from the Korea Centers for Disease Control and Prevention, the number of patients with heat-related illness (HRI) and the number of deaths caused by HRI during the summer in 2018 were 4526 and 48, respectively. These numbers are even higher than those in 2016-2125 patients with HRI and 17 deaths caused by HRI–which was also a hot summer [4]. By the end of the heat wave in 2018, heat waves were included in the official natural disaster list for Korea [5].
Currently, the Korean public health sector lacks an adequate climate change adaptation policy. There is a growing demand to minimize the negative public health impact of climate change by strengthening the governance and response competency of the public health sector. In general, a public policy process consists of policy agenda-setting, formulation, implementation, and evaluation. Since the policy process is not necessarily executed in this order, a policy can be formulated even without a sufficient agenda-setting process [6]. However, accumulating scientific evidence generated by basic research is critical for climate change adaptation policy to be included among important public health policy items. Although many studies on the health effects of climate change have been conducted in Korea, these studies focused mainly on epidemiological research questions, and the epidemiological evidence obtained has not been sufficiently considered as a basis for relevant public health policy. In terms of the policy process, research questions related to agenda-setting have been the most actively investigated; therefore, this study aims to review the current research trend at the agenda-setting stage of climate change adaptation policy in the Korean public health sector. Furthermore, the current study also aims to suggest potential directions of future research so that climate change adaptation can be addressed within the national public health policy.
METHODS
The health impact model suggested in the Intergovernmental Panel on Climate Change (IPCC) Fifth Assessment Report [1] was adapted and revised to define 3 domains of the relationship between climate change and health effects based on the pathways and health effects of climate change (Table 1). Previous studies were systematically reviewed to investigate the current research status of each of the 3 domains.

Three domains of currently-studied topics related to the health effects of climate change and the review methods for each domain
All journal articles, dissertations, and reports that were published by April 30, 2017 were searched. The inclusion and exclusion criteria for the review varied by domain. We used KMBASE, RISS, and KoreaMed as domestic research databases and PubMed, Embase, and the Cochrane Library as international research databases. We also manually searched for publications from the government and research institutes. We included only studies conducted on the Korean general population or on patients in Korea, and we limited the publication languages to English and Korean.
Ethics Statement
This paper is a systematic review so it did not need ethical consideration.
RESULTS
Domain 1: Effects of Ambient Temperature on Death and Cardio-cerebrovascular Disease
The selection process for studies of the effects of ambient temperature on death and cardio-cerebrovascular disease is presented in Figure 1. The search terms are provided in Table 2. More studies within this domain have been conducted than within the other domains. Although the main purpose of this study was to examine trends in published research, it is more informative to review the quality of the studies in detail than to simply count the number of published studies. Therefore, all publication types–journal articles, dissertations, and reports–were included, but the results were restricted to quantitative studies that could be subjected to meta-analysis and used to produce pooled estimates with the results of other studies. The characteristics of the individual study–including study design, population characteristics, temperature variables, temperature units, and thresholds–were extracted, and studies not appropriate for a meta-analysis were excluded.
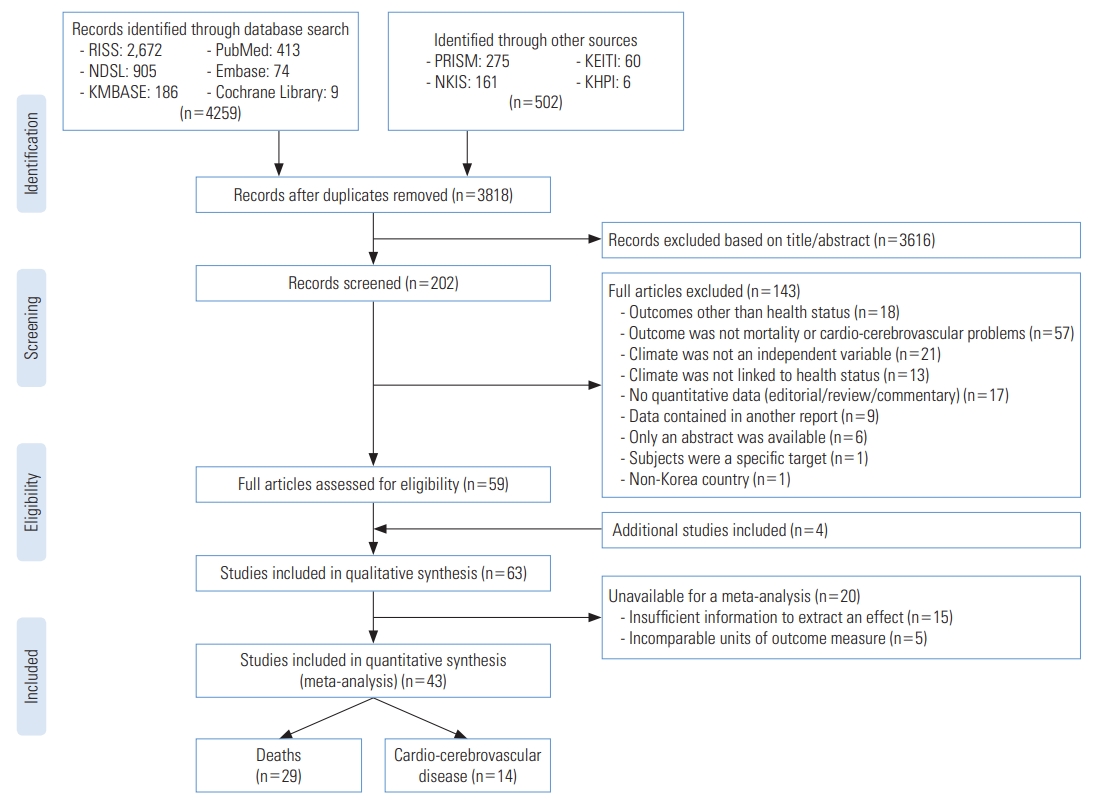
Study selection flow chart for studies of the effects of ambient temperature on death and cardio-cerebrovascular disease. PRISM, policy research database of central and local governments; KEITI: Korea Environmental Industry and Technology Institute; NKIS, National Knowledge Information System; KHPI, Korea Health Promotion Institute.

Climate change and health effect related search terms
Twenty-nine studies were conducted between 2006 and 2016 on the association between ambient temperature and deaths in Korea, and 23 were conducted after 2011 (Figure 2A). More studies were published in international journals (59%) than in domestic journals or institutional sources. Regarding the type of publication, 66% [7-25] of the studies were published as journal articles, followed by dissertations (24%) [26-32] and reports (10%) [33-35]. The proportions of the studies investigating the effect of high temperatures, the effect of low temperatures, the effects of both high and low temperatures, and the effect of diurnal temperature variation were 66%, 7%, 10%, and 17%, respectively. Fourteen studies were conducted on the association between ambient temperature and cardio-cerebrovascular disease in Korea (Figure 2B). More studies were published in international journals (57%) than in domestic journals or institutions. Overall, 57% of the studies were published as journal articles [36-43], 36% were published as dissertations [44-48], and the remaining study was published as a report (7%) [49]. For both death and cardio-cerebrovascular disease, the most frequent publication type was the journal article. This is because the studies available for meta-analysis were generally published by scientific journals.

The number of published studies on the effects of ambient temperature on (A) death and (B) cardio-cerebrovascular disease (domain 1) by year.
Although a large proportion (66%) of the studies evaluated the effect of high temperatures on death or cardio-cerebrovascular disease, it was difficult to estimate stratified risk by age group, region, or cause of death due to the lack of detailed assessments in the original studies. In addition, the temperature indices (such as daily mean, maximum, and minimum temperature) and the operational definition of a heat wave varied across studies. For instance, regarding the definition of a heat wave, 1 study defined a heat wave as an event during which at least 2 consecutive days with daily mean temperatures in the 98th percentile occurred [19], while another study compared the risk of death between the days with daily mean temperatures in the 90th to 99th percentiles and the days with daily mean temperatures in the 50th to 90th percentiles [18]. Additionally, the threshold temperature set by studies varied based on the analysis period, study subjects, or temperature indices. Therefore, that ambient temperature has an effect on death or cardio-cerebrovascular disease in Korea is quite obvious, but the variations in detail make it difficult to discern consistent implications to strategies for intervention against heat waves.
Domain 2: Effect of Ambient Temperature on Other Health Outcomes
The scope of previous studies on the association between ambient temperature and other health outcomes has not been examined. Thus, rather than to analyze characteristics of each study, the current review aimed to identify the scope of the health outcomes addressed in previous studies and to synthesize the pooled evidence quantitatively. For this domain, inclusion was not limited to the studies available for meta-analysis.
The selection process for studies of the effects of ambient temperature on other health outcomes (Supplemental Material 1) aligned with that for the previous domain. All of the publication types–journal articles, dissertations, and reports–were included. The search terms are provided in Table 2. The inclusion of a study was determined based on the title and the abstract. Studies that did not analyze the association between climate and human health, studies for which the original article was not available, and studies for which the subjects were not Korean were excluded.
Among the 57 selected studies, 72% were journal articles, and the rest (28%) were reports or dissertations. The first study was published in 1995, after which only 1 or 2 studies were published per year until 2014. In contrast, between 2014 and 2016, about 10 studies were published every year.
In terms of the types of health outcomes other than death or cardio-cerebrovascular disease, the most frequently published (n=30) health outcome was infectious disease (Figure 3). To be more specific, among studies focusing on vector-borne diseases, the association between ambient temperature and malaria was the most frequently studied [50-60]. Each study had a different range of lag effects. However, the studies had some limitations. The vectors were not sufficiently considered, and assumptions for latent periods, subjects’ traveling, and infection prevention systems were not adequately addressed. Among studies of water- or food-borne diseases, associations between ambient temperature and food poisoning or shigellosis were suggested [61,62], but an insufficient number of studies were performed.
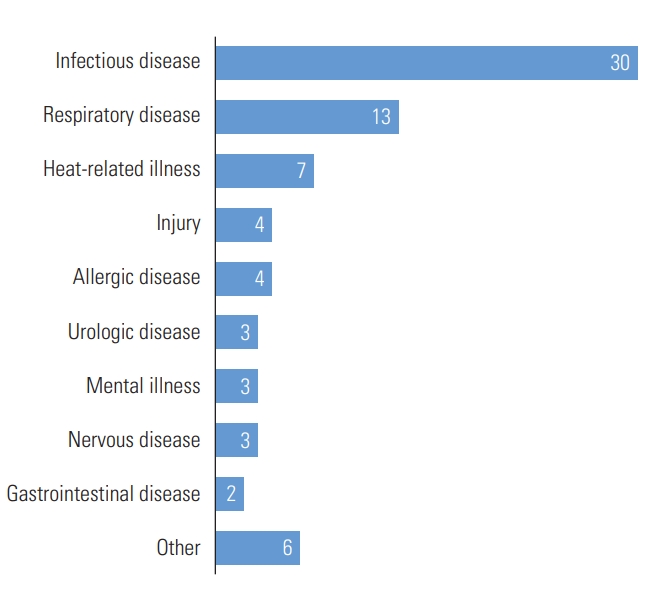
The number of published studies on the effects of ambient temperature on the other health outcomes (domain 2) by health outcomes.
Apart from infectious diseases, several different health outcomes were studied in relation to ambient temperature. Thirteen studies identified an association between ambient temperature and respiratory diseases, and these studies mainly focused on asthma [35,40,41,47,63-65]. However, the direction and the magnitude of the effects were not consistent. Although HRI is typically associated with high temperature, only 7 studies on this topic have been conducted [45,49,66-70]. Studies were also conducted on injury (n=4) [31, 71-73], allergy (n=4) [40,74-76], urinary system diseases (n=3) [31,77,78], mental health (n=3) [79-81], nervous system diseases (n=3) [71,82,83], and digestive diseases (n=2) [71,84].
Domain 3: Effects of Other Climate Factors on Human Health
The national policies for climate change adaptation have focused on temperature-related events, such as heat waves and cold spells. Apart from ambient temperature, it is not clear which climate-related factors can be covered by these policies. For instance, exposure to ultraviolet (UV) light was listed as a health risk in the first Korean national climate change adaptation strategy [85], and the IPCC Fifth Assessment Report [1] mentioned the health risk of UV exposure, but this risk was not included in the second national strategy [86]. Since the scope of the studies on the associations between other climate-related factors and human health was expected to be too broad, only journal articles were included in the review. For this domain, similarly to the second domain, there was no limitation regarding the availability of meta-analysis.
The primary exclusion was conducted based on the title and the abstract, and the secondary exclusion was conducted based on the following criteria: studies (1) not conducted in Korea, (2) with explanatory variables not related to climate factors, (3) with outcome variables not related to human health outcomes, and (4) that were not journal articles (Supplemental Materials 2-7).
A total of 44 studies were included in domain 3, for which the associations between climate factors other than ambient temperature and any health outcomes were assessed. Overall, 82% of them were published in international journals, while 18% were published in Korean domestic journals. As shown in Figure 4, 4 studies on the health effects of natural disasters [58, 87-89] were identified as of April 30, 2017, the studied health effects of which were death (n=2) [87,88], burden of disease (n=1) [58], and water-borne disease (n=1) [89]. Regarding the health impacts of UV exposure, although the major health effects of UV exposure were reported in the IPCC Fifth Assessment Report [1] as melanoma and eye disease, 4 of 5 studies conducted in Korea focused on the mental health outcome of UV exposure [80,81,90,91].

The number of published studies on the health effects of other climate change-related factors (domain 3).
The most frequently assessed climate-related factor in domain 3 in Korea was the health impact of air pollution (n=27). These studies mainly focused on the effects of particulate matter (PM) and ozone on respiratory diseases such as asthma. There were only 2 studies on the outcome of cardio-cerebrovascular disease [37,92], even though patients with cardio-cerebrovascular disease are known to be a population particularly vulnerable to PM exposure.
Seven studies examined changes in the ecology of infectious disease vectors, 4 of which dealt with malaria [50,55,93,94]. Although some studies were classified as domain 1 (studies on the effects of ambient temperature on the other health outcomes), if more specific keywords were used for certain topics such as ‘vector’ or ‘mosquito’, fewer studies were identified using the term. Few studies were conducted to identify changes in the ecology of microorganisms (n=2) [95,96]. This might be because keywords like ‘vector’, ‘food’, and ‘water’ were not considered important keywords in the titles or abstracts of these studies. As previously described, in the context of climate change research, studies on vector-borne diseases focused on the effects of ambient temperature without sufficient consideration of the vector ecology.
Lastly, there were 6 studies of mental health outcomes, 4 of which assessed the effect of number of hours of sunshine [80, 81,90,91]. These studies mainly evaluated the effects of temperature, but indices utilized for exposure to ambient temperature are high temperatures (or heat waves), low temperatures (or cold spells), and diurnal temperature variation, but not hours of sunshine.
DISCUSSION
The primary purpose of this study was to review the amount of evidence that has been gathered at the agenda-setting stage of the policy process for climate change adaptation in the Korean public health sector. The existence of health effects of climate change has been proven by studies of Korean populations as well as those conducted in foreign countries. Nevertheless, climate change adaptation policy in the public health sector has not been treated as a high-priority national policy. Although several factors are involved in placing an issue under consideration as a national policy agenda item, scientific evidence is one of the most important requirements. Thus, for the health impact of climate change to become a major national policy agenda item in Korea, it is necessary to evaluate the status of the current scientific evidence regarding the health impacts of climate change and to identify areas that need more scientific research.
The scope of health outcomes that can be attributed to climate change is so extensive that it is difficult to report as one generalized result. In Korea, the main focus of the current adaptation policy has focused on responses to heat waves, and the most frequent area of research was that which assessed the health impacts of ambient temperature, especially the impact on death or cardio-cerebrovascular diseases. Nonetheless, from the review of the scientific evidence, it is hard to determine the urgency and the importance of the target, criteria, and scale of the adaptation strategy. Specifically, it is difficult to apply the major adjusting variables in the assessment of general health impact, and consequently, the results of the studies involved a significant amount of assumptions and uncertainties.
As for the effects of ambient temperature on other health outcomes, studies of infectious diseases have been most actively conducted, but these mainly focused on malaria, which occurs relatively infrequently and is regarded as being properly managed in Korea. Also, since infectious diseases are closely related not only to individual characteristics, but also to social or environmental factors, there are more uncertainties related to infectious disease outcomes than to death or cardio-cerebrovascular disease. For health outcomes except for death, cardio-cerebrovascular diseases, and infectious diseases, an insufficient number of studies were conducted to address the corresponding health risks in Korea.
Subareas of climate change include changes in ambient temperature, air pollution, natural disasters, vector-borne disease, and water- and food-borne disease. While many studies have been published regarding changes in ambient temperature, for the other subareas of climate change, little has been reported. Infectious disease outcomes were studied only in relation to changes in ambient temperature, and few studies have been conducted on disasters. Although there were a considerable number of studies on air pollution, it cannot be said that sufficient scientific evidence exists, both because there are many different pollutants and because corresponding health effects manifest with high complexity.
The studies evaluated in the current review can be considered research at the agenda-setting stage in only a narrow sense. This is because, in general, agenda-setting encompasses the steps required to identify the problem, define the problem, and call public attention to the problem, influencing the political agenda [6]. In other words, the studies on the health effects of climate change have defined the problem, but they have not yet addressed the issues in the policy-making context.
At the agenda-setting stage, defining a problem is not the end of the stage. Only when the general public and policy-makers acknowledge the problem and when policy-makers start to discuss possible solutions is the problem finally becoming part of the agenda [6]. It is difficult to turn a defined problem into an agenda item using basic scientific research alone. The scientific evidence from the results should be refined for discussion by policy-makers in the following step. To achieve this goal, communication channels for researchers, national public health authorities, and policy-makers are needed. Through these channels, the involved parties can consistently discuss the health problems that must become part of the public agenda.
For future research to become a basis for climate change adaptation policy in the public health sector, the following changes are needed. First, we recommend the sharing and development of databases that measure exposure to climate-related factors and health outcomes. There is no single standardized method to estimate the health effects of climate change, and diverse study designs are needed to assess various aspects of the health impact of climate change. However, the researchers behind many studies have had no choice but to apply limited study designs due to the lack of diverse databases. As limited databases have been analyzed repeatedly, the underestimation or overestimation of effects or overlapping similar effect estimates should be cautiously examined. To be specific, there is a paucity of databases that represent the exposure or response characteristics of individuals or population groups. As a result, it is challenging to assess the health effects of an exposure multidimensionally and to find potential intervention points from the study results. Therefore, developing databases that adequately reflect the exposure status and socioeconomic characteristics of individuals and populations is strongly suggested.
Second, the national government should assess climate change-related health effects and set the priorities for adaptation to climate change. In the United States, the Centers for Disease Control and Prevention suggested criteria to decide the prioritization of health problems. The criteria included the magnitude of the problem, the seriousness of the problem, the availability of the current intervention, economic damage, and public interest [97]. So far, the subject of research that assesses the health impact of climate change has been decided by the researchers’ interest. Thus, it is hard to know how long it will take to fully determine the previously-referenced criteria for determining policy priorities. International organizations like the IPCC and the WHO have already delineated the health problems that are highest-priority. Furthermore, in the United States, the Centers for Disease Control and Prevention [98] and the US Global Change Research Program [99] have reported the health impacts of climate change. In the United Kingdom, a climate change risk assessment is conducted every 5 years, and the results of the assessment are utilized to develop adaptation strategies in the following year [100]. The United Kingdom government defines the major health problems attributable to climate change and revises the scope of the health effects in accordance with the situation. In other words, the priority of agenda items for national climate change adaptation strategies should be determined as part of a government initiative. In addition, the government should develop and support research topics needed to develop policies.
CONCLUSION
Many studies evaluated the effects of temperature on death and cardio-cerebrovascular disease in Korea. However, there was a limit to the use of these studies in the policy process for climate change adaptation. Not only were there not many studies of effects of ambient temperature on other health outcomes and effects of other climate factors on human health, but the results of these studies were inconsistent. Efforts should be made to minimize health problems according to climate change in government health policy. Therefore, the amount and quality of research that can support health policies should be improved.
SUPPLEMENTAL MATERIALS
Supplemental materials are available at https://doi.org/10.3961/jpmph.19.326.
Study selection flow chart for studies of the effects of ambient temperature on other health outcomes. RISS, Research Information Sharing Service; NDSL, National Digital Science Library; KMBASE, Korean Medical Database; PRISM, policy research database of central and local governments; KEITI: Korea Environmental Industry and Technology Institute; NKIS, National Knowledge Information System; KHPI, Korea Health Promotion Institute.
Study selection flow chart for studies of the effects of other climate factors on human health- natural disaster. RISS, Research Information Sharing Service; NDSL, National Digital Science Library; KMBASE, Korean Medical Database.
Study selection flow chart for studies of the effects of other climate factors on human health- UV light. RISS, Research Information Sharing Service; NDSL, National Digital Science Library; KMBASE, Korean Medical Database.
Study selection flow chart for studies of the effects of other climate factors on human health- air pollution. RISS, Research Information Sharing Service; NDSL, National Digital Science Library; KMBASE, Korean Medical Database.
Study selection flow chart for studies of the effects of other climate factors on human health- vector-borne disease. RISS, Research Information Sharing Service; NDSL, National Digital Science Library; KMBASE, Korean Medical Database.
Study selection flow chart for studies of the effects of other climate factors on human health- water/food-borne disease. RISS, Research Information Sharing Service; NDSL, National Digital Science Library; KMBASE, Korean Medical Database.
Study selection flow chart for studies of the effects of other climate factors on human health- mental health. RISS, Research Information Sharing Service; NDSL, National Digital Science Library; KMBASE, Korean Medical Database.
Notes
CONFLICT OF INTEREST
The authors have no conflicts of interest associated with the material presented in this paper.
FUNDING
This article was funded by Korea Institute for Health and Social Affairs.
ACKNOWLEDGEMENTS
This article was based on a report (Chae et al. Development of evidence-based health policy response to climate change. Sejong: KIHASA; 2017).
Notes
AUTHOR CONTRIBUTIONS
Conceptualization: SMC. Data curation: SMC, DK. Formal analysis: SMC, DK. Methodology: SMC. Funding acquisition: SMC. Writing- original draft: SMC, DK. Writing - review & editing: SMC, DK.