Barriers to Health Service Utilization Among Iranian Female Sex Workers: A Qualitative Study
Article information

Abstract
Objectives
In most countries around the world, sex work is an illegal activity. Female sex workers (FSWs) in Iran hide their identities, and they are known to be a hard-to-reach population. Despite free access to HIV testing, fewer than half of FSWs receive HIV testing. The purpose of this study was to characterize the reasons for which FSWs do not seek testing at drop-in centers (DICs) and voluntary counseling and testing (VCT) centers in Iran.
Methods
A qualitative study was conducted in 2016. The participants were 24 FSWs who received services at VCT centers and DICs for vulnerable females in the north of Iran and 9 males who were the clients of FSWs. In this study, we made use of purposive sampling and carried out a thematic analysis.
Results
We found 4 major and 6 minor themes. The major themes were: fear of being infected (with HIV), stigma, indifference, and knowledge.
Conclusions
Despite the significant efforts made by the government of Iran to establish and expand DICs for vulnerable females, the number of FSWs receiving services at these centers has not been very considerable. Consequently, by introducing and implementing training programs for peer groups, it may be possible to take steps toward establishing strategic programs for the control and prevention of HIV/AIDS.
INTRODUCTION
The manner in which sex work is carried out and its legal status are different in various regions. In socioculturally conservative countries, as well as in Islamic countries in the Middle East, female sex workers (FSWs) are considered to be “social evils” and “norm-breakers.” Therefore, they are often excluded from society, which puts them at risk of social harm and endangers their social welfare, access to health care services, and reproductive health rights.
FSWs are known to be a key population that plays an important role in the dynamics of HIV transmission, and the Joint United Nations Programme on HIV/AIDS reported the worldwide HIV prevalence among this population to be approximately 11.8% in 2015 [1]. Due to the types and the number of FSWs’ sexual partners or clients (i.e., their sexual network), they can contribute to an increased rate of HIV transmission. Nonetheless, their clients, as the bridge population that transmits the infection to other people in society, play the most important role [2,3]. It is estimated that approximately 80 000 FSWs live in Iran, of whom 4.5% are HIV-positive [4]. However, this information is derived from estimates obtained from drop-in centers (DICs) and voluntary counseling and testing (VCT) centers, which means that this number is likely to be an underestimate [4].
Currently, the AIDS epidemic is concentrated in certain subgroups of the population in Iran. More than 5% of the high-risk population and less than 1% of the general population is affected by this infection [2]. Meanwhile, according to the latest (2016) report of the Ministry of Health and Medical Education of Iran, approximately 32 000 HIV-positive individuals have been identified [5]. However, in a study published in 2011, researchers estimated that this number would increase to 106 000 cases by the end of 2014 [4]. Taken together, these findings indicate that most HIV-positive individuals are not aware of their disease status, and therefore act as hidden or potential sources of HIV transmission. The third wave of HIV transmission is reported to be moving through unprotected sexual intercourse [4], and the Ministry of Health and Medical Education of Iran has reported that 42% of cases of HIV transmission in the beginning of 2016 took place through sexual intercourse [6].
A national monitoring and evaluation program conducted in 2009 throughout 10 provinces in Iran showed that FSWs who received HIV testing and counseling services at VCT centers and DICs in 2007 and 2008 had HIV positivity rates of 5 and 7%, respectively [7]. In 2007 and 2008, 14.0 and 17.5% of FSWs, respectively, received counseling at DICs and VCT centers [8]. Moreover, despite free access to HIV testing for FSWs, fewer than half of them received HIV testing in 2010 [9]. In a study of FSWs living in Tehran in 2007, 59.3% of them stated that they know where to go to get an HIV test [10]. Studies have found that the majority of FSWs visit private health centers to receive health and treatment services. However, these centers do not provide regular reports of the services they provide [11-13]. One of the most important reasons why FSWs do not visit DICs and VCT centers for health and treatment services is the discrimination and stigma associated with HIV infection. This finding has been reported in the majority of the studies carried out to investigate this issue [9,14-16]. Fear of identification and punishment for engaging in sex work, the stigma conveyed by the service providers, distance to the centers, and fear of HIV testing have been reported as major obstacles in many studies [9].
In most countries around the world, sex work is an illegal activity. Iran is a country in which sex work is considered to be a crime with severe punishments. However, although sex work is associated with important public health issues, FSWs in Iran hide their identity, and they are known to be a hard-to-reach population [9]. Initially, due to the cultural limitations in providing health services to FSWs, a goal of providing counseling and voluntary testing to 17% of this population seemed appropriate. However, because of the increased prevalence of HIV infection in FSWs and the risk of a concentrated epidemic emerging among them, which could cause HIV to spread among the general population, broader planning to increase coverage for preventive and diagnostic services for these groups is necessary [8].
In order to successfully implement preventive and surveillance programs for HIV/AIDS, it is necessary to have access to high-risk groups to ensure the optimal efficacy of the programs. Therefore, peer groups can be of great significance for the success of such programs. The purpose of this study was to characterize the reasons for which FSWs do not seek counseling and testing services at DICs and VCT centers in Iran through qualitative methods.
METHODS
A qualitative study was conducted in 2016, and the participants were 24 FSWs who received services at VCT centers and DICs for vulnerable females in the north of Iran and 9 male clients of FSWs. Forty-nine females who received services at these centers were initially invited to participate in the study, and 24 of those females met the inclusion criteria. Twenty-one male clients of FSWs were initially invited, but only 9 met the inclusion criteria. The inclusion criteria for the FSWs were as follows: being a female 18 years or older, having sex work experience or being the madam (i.e., manager) of other FSWs for at least 1 year, being the acquaintance or friend of 5-7 FSWs who had not received services at these centers; and completing the informed consent form to participate in the study. The inclusion criteria for male clients of FSWs were as follows: being a male 18 years or older; having had at least 1 sexual contact with FSWs per month during the last year; being familiar with 5-7 FSWs who had not received services at these centers, and completing the informed consent form to participate in the study. Before starting this study, all participants were informed about the topic and purpose of the study. In addition, they were informed that they were free to participate in the study or to discontinue participation, and written informed consent was provided by each participant.
First, the interview guide was prepared and provided to the interviewees. Then, semi-structured in-depth interviews were conducted with the participants. They were individually interviewed in a private room. Participants were asked for their opinions about the factors that prevented FSWs from visiting VCT centers and DICs for services. Two interviewers (1 male and 1 female) who were trained and experienced in this context (VCT center and DIC staff) conducted the interviews, which were recorded. Data were gathered through the recordings of the interviews. Then, notes taken about the interviews and the data were coded by 2 experts based on the purposes of the study, and the themes were identified. In each coding session, key and significant expressions in each text were identified in relation with the topic and the individual. Coding was conducted in 3 stages:
1) free coding (first stage), 2) axial coding (second stage), 3) selective coding (third stage)
In this study, we used purposive sampling. After 33 interviews (24 females and 9 males), we were theoretically saturated, and no additional information emerged after the 24th interview. The interviews were conducted in a way that was suitable for sensitive issues. In-depth interviews conducted by the first author lasted between 1 and 4 hours, and several audit were held prior to the interview to build rapport with the interviewee. A female interviewer conducted the interviews with the FSWs, and a male interviewer interviewed the male clients. The data were analyzed using content analysis. In this type of qualitative analysis, the data are minimized and structured in an orderly manner. In addition, repetition, occurrence, meaning, and the relationships between certain words in the transcripts and concepts were determined. In this stage, the content of the message that needed to be analyzed was defined. Moreover, attempts were made to recognize the units of content analysis. The interviews were read several times, and then the participants’ ideas and experiences with regard to barriers preventing FSWs from receiving services at DICs and VCT centers were extracted and saved as text. After that, the coding stage was conducted.
Factors such as fear, stigma, indifference, and lack of knowledge are very sensitive items in Iran, which prevents FSWs from visiting these centers for counseling and testing. It is essential to consider the importance of these major themes and their tangibility, especially in tourist areas in tourist areas in northern Iran along the Caspian Sea.
Additionally, sub-themes were extracted from the same questions as the main themes.
Ethical Considerations
This study received an ethical and project code (25463) from the Vice-Chancellery of Research of Iran University of Medical Sciences. All participants provided written consent to participate in the study and all interviews were conducted anonymously.
RESULTS
Demographic Features
The female participants’ age range was from 25 to 39 years, and the male participants’ age range was from 23 to 35 years. The females’s age of first sexual contact was from 12 to 34, and that of the males was from 16 to 21 years. The average age of first sexual contact for the females and males was 20.5 and 18.0, respectively. The females’s average age at beginning sex work was 22.5 years (range, 12-34). A minority of the females (23.8%) were not local; the rest, as well as the male clients, were all local. Of the FSWs, 52.4% were divorced, 19.0% were married, 19.0% were single, and 9.6% were in a sigheh (temporary marriage) relationship. Of the males, 55.6% were single, 22.2% were separated from their family, 11.1% were divorced, and 11.1% were married. In 81.0% of cases, the place for having sexual intercourse was determined by the clients, while in the remaining cases, it was determined by the FSWs. The females methods for finding clients varied, including through cell phones and the Internet (38.0%), introductions from friends and other clients (14.3%), on the streets (19.0%), and other ways (28.7%). Of the FSWs with marriage experience, 41.2% had experienced 2 or more marriages.
Qualitative Findings
A thematic analysis was conducted of the 24 FSWs and 9 clients, and the results are presented in Table 1 by main and minor themes. The interpretation of the thematic analysis was as follows:
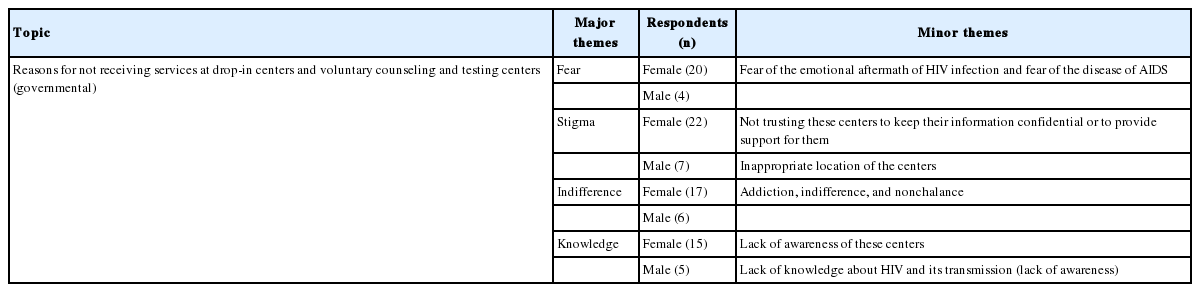
Thematic analysis of barriers to health service utilization by female sex workers according to major and minor themes
Fear of being infected (HIV)
One of the main reasons why FSWs were not willing to receive counseling and testing at DICs and VCT centers, which provide health and treatment services, was that they feared being officially diagnosed with an HIV infection; therefore, for receiving services, they preferred visiting other centers (private) that provide anonymous testing. Regarding this issue, one of the participants stated:
I fear being infected with the disease. If I find out that I am infected, I may get depressed or lose my hopes for living, and so on.
Another participant stated:
I have a friend who has a lot of sexual relations and I know her circumstances. I asked her to come to these places and have some tests done. Their services are free, and you don’t need to pay anything. But she always says, “Drop it; I’m afraid, I fear being infected.”
Stigma (low quality of drop-in centers and voluntary counseling and testing services)
During the interviews, most of the participants mentioned confidentiality and the supportive services offered by the centers as major reasons for not visiting them for testing and counseling. In this regard, one of the participants stated:
The main reason why people do not visit these centers is that they cannot trust them. They think that these centers will reveal their secrets or that their names will be reported somewhere.
Another issue identified by some participants was the inappropriate location of these centers, which can attach stigma to the people visiting them for services. Due to this stigma, most HIV-positive individuals postpone visiting these centers for surveillance or treatment, and they do not follow their surveillance programs correctly.
Another participant stated:
Going to these centers is often very difficult for us. This center is an example, because in front of the entrance, there is a taxi stand. The drivers look at whoever comes in, and they ask: What is this place? Why are these females visiting this center? What is their problem? Who are they? What’s wrong with them? And so many other questions!
Indifference
Many drug-addicted females, due to their addiction, do not use condoms and do whatever their clients desire. Most such FSWs described experiencing physical injuries, such as sexual violence and other types of violence. They stated that when the clients became aware of the FSWs’ addictions, they misuse them and do not care about whether the FSWs ask to use a condom. Moreover, drug-addicted FSWs stated that using a condom was not very important for them and that obtaining drugs was the only significant issue that they thought about at the time [17].
Most of the participants in the present study confirmed these issues. One stated:
These people do not care about their health. That is why they do not set aside time to come here and receive the education needed to change their lifestyle and behaviors.
Knowledge
Some of the participants stated that most people were not aware of these centers or they did not know where the centers were. In this regard, a participant said:
You know, some of these people do not know anything about these centers or the places that provide various services. Maybe there are not enough advertisements. People don’t know about these centers. You know, they don’t know that they can come here to receive treatment, receive counseling, talk about their problems, or at least be trained for a job or profession.
One of the greatest challenges for various groups throughout society, especially high-risk groups, is insufficient knowledge about HIV/AIDS and its transmission routes. In this regard, another participant stated:
These people are not aware of the risks related to their activities. For example, they don’t know anything about the consequences of having sexual contacts with various people without using a condom.
DISCUSSION
In this study, 4 main themes were identified: fear, stigma, indifference, and knowledge.
We found that a major reason why FSWs do not visit DICs and VCT centers to receive services is their fear of being infected with HIV/AIDS, and their fears of its mental and emotional aftermath.
Due to the fear of becoming an outcast and the other social consequences of HIV infection, these groups reject the possibility of having such a disease and they do not seek out voluntary HIV testing, which is known to be a significant preventive measure that can be taken against HIV and its spread throughout society [18,19]. The fear of being identified as an infected person is prevalent in most countries. Thus, FSWs’ fear of being infected is a reason why they do not visit DICs for testing [13, 20,21].
Additionally, the participants expressed concerns about stigma and discrimination in the form of a lack of confidence in these centers, particularly regarding confidentiality and support services. Similarly, other studies have found stigma, discrimination, and lack of confidentiality to be barriers preventing FSWs from visiting such centers [22-24]. In addition to HIV stigma and discrimination, which create barriers for patients and high-risk individuals, the possibility that access to and utilization of HIV prevention services may be subsequently disrupted can lead to severe psychological injury in these people. Studies have indicated that HIV-infected individuals, as well as those suspected to have HIV, who have been stigmatized or discriminated against can lose their self-esteem and suffer from depression and hopelessness [25,26]. Moreover, stigma and discrimination can indirectly lead to the social isolation of people with HIV or suspected to have HIV.
It is a reality that HIV-positive individuals can be isolated from other people as part of various HIV control measures [27]. Stigma and discrimination cause HIV-positive people to be viewed as a problem, not as the solution for this epidemic. Moreover, by not allowing people with HIV to participate in programming for AIDS control measures, we lose opportunities for managing AIDS prevention and the AIDS epidemic itself [28,29].
Participants also identified a lack of awareness of the existence of these centers, as well as of the routes of HIV transmission. Similarly, in some other studies conducted in Iran and certain other countries, one of the main reasons for which people did not visit these centers for services was reported to be their lack of knowledge about the disease or their unawareness of centers that provide HIV-related services [30-32]. Moreover, according to the most recent population-based study of Iranian youths’ knowledge, attitudes, and practices, more than 60% of the participants did not have enough knowledge about AIDS, and they believed that no supportive measures were provided by state centers [33]. Nonetheless, increasing awareness of HIV/AIDS can be a powerful tool for improving positive attitudes throughout society and facilitating the adoption of methods to prevent HIV transmission. Obtaining a clear understanding of the knowledge, attitudes, and practices of each society can make a highly significant contribution for strategic programming aimed at controlling and preventing HIV infections [34].
One of the most important limitations of this study is the lack of access to FSWs who did not visit these centers. Due to the severe legal and extra-legal consequences of sex work in Iran, as it is both a crime and a socially stigmatized behavior, this population is difficult to access. Moreover, FSWs may not provide accurate information to health service providers. For these reasons, in this study, people who were close to such FSWs were selected for interviews.
Despite the significant efforts made by the Iranian government to establish and expand VCT centers and DICs for vulnerable females, the number of FSWs receiving services at these centers has not been very considerable. This issue is one of the greatest limitations in implementing strategic programs for the prevention and control of HIV infection [8].
For the reasons we have discussed, the most hidden and hard-to-reach populations in society, which can be exposed to sexually transmitted diseases, especially HIV/AIDS, may not be easily accessible or visible. Based on the results of the present study, factors that prevent FSWs from accessing HIV counseling and testing services should be identified and minimized. Therefore, various methods, such as increasing knowledge and providing the appropriate social context by gaining access to high-risk groups, can be very effective measures in practice. Consequently, by introducing and implementing training programs for peer groups in Iran and other countries facing similar challenges, it may be possible to take steps towards establishing strategic programs for the control and prevention of HIV/AIDS.
ACKNOWLEDGEMENTS
We would like to express our special thanks to the Vice-Chancellor of Health of the Mazandaran University of Medical Sciences and the Vice-Chancellor of Research of Iran University of Medical Sciences, who helped us carry out this study. This study is part of an approved project (code: 25463) at Iran University of Medical Sciences.
Notes
CONFLICT OF INTEREST
The authors have no conflicts of interest associated with the material presented in this paper.