Gender Differences in Hypertension Control Among Older Korean Adults: Korean Social Life, Health, and Aging Project
Article information
Abstract
Objectives:
Controlling blood pressure is a key step in reducing cardiovascular mortality in older adults. Gender differences in patients’ attitudes after disease diagnosis and their management of the disease have been identified. However, it is unclear whether gender differences exist in hypertension management among older adults. We hypothesized that gender differences would exist among factors associated with hypertension diagnosis and control among community-dwelling, older adults.
Methods:
This cross-sectional study analyzed data from 653 Koreans aged ≥60 years who participated in the Korean Social Life, Health, and Aging Project. Multiple logistic regression was used to compare several variables between undiagnosed and diagnosed hypertension, and between uncontrolled and controlled hypertension.
Results:
Diabetes was more prevalent in men and women who had uncontrolled hypertension than those with controlled hypertension or undiagnosed hypertension. High body mass index was significantly associated with uncontrolled hypertension only in men. Multiple logistic regression analysis indicated that in women, awareness of one’s blood pressure level (odds ratio [OR], 2.86; p=0.003) and the number of blood pressure checkups over the previous year (OR, 1.06; p=0.011) might influence the likelihood of being diagnosed with hypertension. More highly educated women were more likely to have controlled hypertension than non-educated women (OR, 5.23; p=0.013).
Conclusions:
This study suggests that gender differences exist among factors associated with hypertension diagnosis and control in the study population of community-dwelling, older adults. Education-based health promotion strategies for hypertension control might be more effective in elderly women than in elderly men. Gender-specific approaches may be required to effectively control hypertension among older adults.
INTRODUCTION
Hypertension is one of the most prevalent chronic diseases that acts as a modifiable risk factor for cardiovascular disease (CVD), stroke, and kidney disease [1]. Preventing CVD, a leading cause of death that accounts for up to 35% of all-cause mortality in Western countries and 30% of all global death [2], has been a global priority for health policy [3]. Currently, highly cost-effective antihypertensive medications are available, and taking antihypertensive medication is the most important factor associated with an improvement in blood pressure (BP) control among adults with diagnosed hypertension [4]. Therefore, being aware of and understanding hypertension as well as adhering to antihypertensive treatments and lifelong healthy behaviors (e.g., not smoking, avoiding binge drinking, being more physically active, and eating a healthy diet) are critical for hypertension control.
Globally, undiagnosed and uncontrolled hypertension are highly prevalent, and a major barrier to the reduction of CVD [5]. According to data from the National Health and Nutritional Examination Surveys (2011-2012), the prevalence of hypertension is about 30% among adults in the USA, and approximately half of these cases of hypertension are uncontrolled [6]. As the prevalence of hypertension increases with aging, about two thirds of older adults become hypertensive [7]. A recent Korea National Health and Nutrition Examination Survey (KNHANES) also showed similar results, with 64.7% of Koreans aged 65 and older having hypertension but only 54.4% of them having controlled hypertension [6]. The asymptomatic nature of hypertension, together with the absence of distress or acute functional changes, may not motivate older adults to seek medical treatment. However, suboptimal management of hypertension in older adults can eventually result in CVD morbidity leading to frequent hospitalization [8], higher health care costs [9], and lower quality of life [10,11]. Considering the rapid increase in the proportion of older adults in the population and the high rate of suboptimal hypertension management in South Korea, controlling BP is a key step in attempts to reduce the CVD burden in older age.
Gender differences have been shown in the development and management of hypertension [4,12-14]. Women are more likely to develop a steep age-related increase in arterial stiffness after menopause [15] and are more likely to have uncontrolled hypertension than men [12,16,17]. Although the treatment benefit of antihypertensive agents does not differ between men and women [18], hypertensive women are less likely to achieve recommended BP goals even with a significantly higher use of antihypertensive drugs [12]. However, whether these gender discrepancies in controlling hypertension exist in older adults is not clear because health-related behaviors such as being screened by a healthcare professional, seeking advice, and attending educational sessions change with age as well as gender [19]. Moreover, limited evidence is available for gender differences in hypertension control among community-dwelling older adults.
We hypothesized that gender differences would exist among factors associated with hypertension diagnosis and control among community-dwelling, older adults. Exploration of gender differences in patients’ awareness of their BP level, attitudes to health screening, and clinical features could be an important step towards establishing gender-specific strategies to promote adherence to treatment and lifelong preventive health behaviors in this community.
METHODS
Design and Subjects
This study was conducted as a part of the Korean Social Life, Health, and Aging Project (KSHAP). The KSHAP aimed to recruit the entire population of adults aged 60 years or older, and their spouses, living in a single township on Gangwha Island, Korea. As of January 2013, the total population consisted of 1864 individuals in 871 families. With the aid of the township office and after performing a pilot study, a total of 860 people were identified as the target population of the KSHAP. Of these 860 adults, 814 people (94.7% response rate) completed face-to-face interviews from December 2011 to March 2012 [20]. All KSHAP participants were also invited to attend health examinations, and 698 people (85.7% of KSHAP participants, 81.1% of target population) received health examinations at a public health center (n=533) or at home (n=165) [21]. Individuals for whom data on BP checkup behaviors (n=15) or physical examination (n=30) was missing were excluded. Therefore, we included data from 653 older adults in the current study. Data from surveys and BP measurements were collected at the public health center or respondents’ homes by trained interviewers using a standardized questionnaire and protocol. The institutional review board of Yonsei University approved this study (YUIRB-2011-012-01), and each participant provided informed consent.
Measurement of Hypertension
Hypertension categories were derived from self-report and BP measurement at the health examination as suggested by Cornwell and Waite [22]. Physician-diagnosed hypertension or diabetes were identified by self-report by asking participants if their physician had ever told them that they had hypertension or diabetes. Resting systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured at least twice with the oscilloscopic method using an automatic sphygmomanometer (Carescape Dinamap V100; GE Healthcare, Milwaukee, WI, USA). Prior to each measurement, all participants rested for at least 5 minutes in a seated position, and the cuff size was adapted to their right upper arm. If the first and second measurements differed by ≥10 mmHg for either SBP or DBP, additional measurements were performed, and the average of the last two measurements were used for analysis. Elevated BP was defined as SBP ≥140 mmHg or DBP ≥90 mmHg for participants without diabetes, and as SBP ≥130 mmHg or DBP ≥80 mmHg for participants with a self-reported diabetes diagnosis. Self-reported hypertension diagnosis and BP measurements were used to categorize hypertensive participants as having undiagnosed hypertension (no physician diagnosis, but elevated measured BP), uncontrolled hypertension (physician-diagnosed hypertension with elevated measured BP), or controlled hypertension (physician-diagnosed hypertension without elevated measured BP).
Covariates
Standing height and body weight were measured to the nearest 0.1 cm using a stadiometer and 0.1 kg using a digital scale, respectively. Body mass index (BMI) was calculated as kilograms per meters squared. Blood samples were collected from the antecubital vein of participants who had fasted at least 8 hours to measure total cholesterol and high-density lipoprotein cholesterol. In addition, data on socio-demographic information (age, education, occupation, co-resident partners, etc.), health behaviors (smoking status, alcohol intake, current use of antihypertensive agents, antihypertensive medication adherence, awareness of one’s own BP level, and frequency of BP checkups per year), and perceived health status were collected using the standardized questionnaire. The 10-year risk of coronary heart disease was calculated based on the Framingham point scores [23].
Statistical Analysis
The differences in general characteristics between participants with and without hypertension were analyzed using independent t-tests for continuous variables and chi-square tests for categorical variables. All analyses for participants with hypertension were performed separately for men and women. For these gender-specific analyses, chi-square tests for categorical variables and t-tests or analyses of variance with a post-hoc analysis using Scheffe methods for continuous variables were performed. Multiple logistic regression models were used to identify factors which contribute to hypertension diagnosis among people with hypertension, and to identify factors which contribute to hypertension control among people with diagnosed hypertension. Independent variables in the logistic model included age, BMI, total cholesterol, high-density lipoprotein cholesterol, education, cigarette smoking, comorbid diabetes, BP level awareness, and the number of BP checkups per year. All analyses were performed using PASW Statistics version 18.0 (SPSS Inc., Chicago, IL, USA) and Stata 12.0 (StataCorp., College Station, TX, USA), and a two-sided p-value of less than 0.05 was considered to be statistically significant.
RESULTS
Table 1 compares variables in people with hypertension and without hypertension. Among the 653 participants, 433 (66.3 %) had hypertension. People with hypertension were more likely to be older, and less likely to be educated and live with a partner. There were no significant differences in health behaviors such as smoking and alcohol intake or in diabetes comorbidity between non-hypertensive and hypertensive participants. However, hypertensive participants were more likely to know their own BP level (71.8% vs. 58.6%, p=0.001), check their BP more often (19.0 times per year vs. 8.8 times per year, p<0.001), and perceive their health as bad (49.4% vs. 33.2%, p<0.001) compared to non-hypertensive participants. Table 2 shows the characteristics of hypertensive participants by gender. Hypertensive men were more likely to be educated, have a job, live with a partner, smoke cigarettes and drink alcohol, but less likely to have a worse perception of their health than hypertensive women. A total of 76.9% (72.2% in men and 79.9% in women) of hypertensive participants reported that they had been previously diagnosed with hypertension. The rate of controlled hypertension was 55.3% (57.4% in men and 53.6% in women) among those with diagnosed hypertension and 42.3% (41.4% in men and 42.8% in women) among all individuals with hypertension.
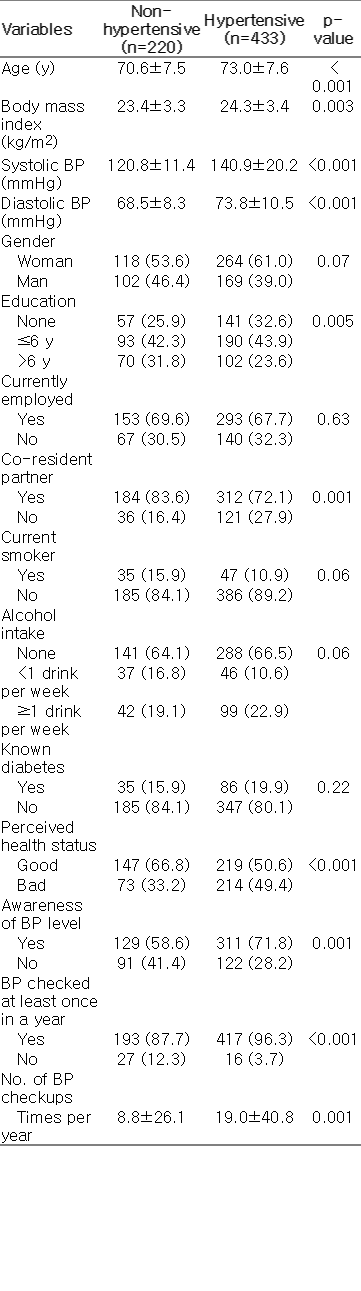
Characteristics of participants according to hypertension status (n=653)
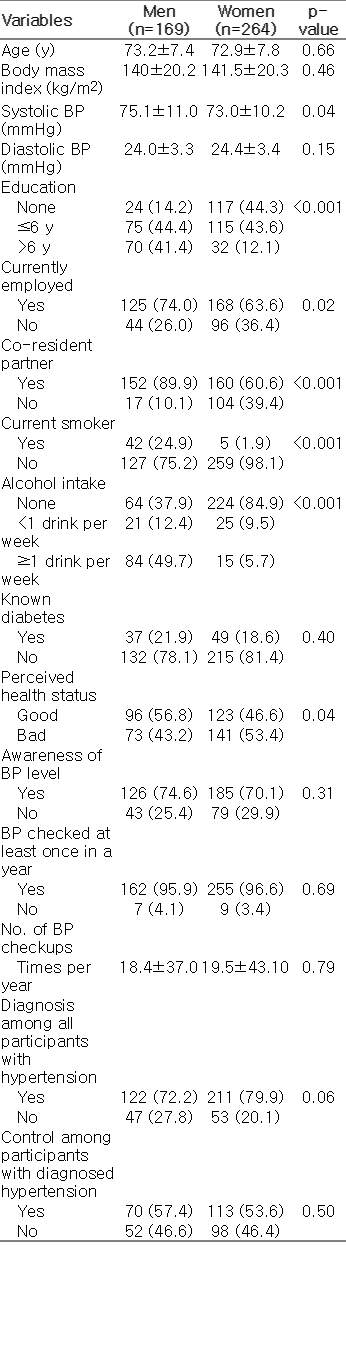
Gender comparison among participants with hypertension (n=433)
Table 3 compares undiagnosed, uncontrolled, and controlled hypertension separately for men and women. Diabetes was more prevalent among men with uncontrolled hypertension (42.3%) than it was among men with controlled (15.7%) or undiagnosed (8.5%) hypertension. Similarly, diabetes was more frequent in women with uncontrolled hypertension (31.6%) than in women with controlled (11.5%) or undiagnosed (9.4%) hypertension. Higher BMI was significantly associated with uncontrolled hypertension only among men with hypertension, whereas lower educational level was associated with uncontrolled hypertension among women with hypertension. The estimated 10-year coronary heart disease risk was significantly higher in participants with uncontrolled hypertension than in those with undiagnosed or controlled hypertension in both men and women. Self-reported health status, antihypertensive medication use, and antihypertensive medication adherence did not differ by hypertension status in either men or women. Awareness of BP level and the frequency of BP screening had different associations with hypertension status for men and women. Women with undiagnosed hypertension were less likely to know their BP level and check their BP level than women with uncontrolled or controlled hypertension. However, neither the awareness of BP level nor the number of BP checkups was associated with hypertension status in men. The number of BP checkups was not significantly different between the three groups of hypertension status in men (p= 0.085). However, when we merged the undiagnosed and uncontrolled hypertension groups, men with controlled hypertension checked their BP more frequently than those with undiagnosed or uncontrolled hypertension (25.8 vs. 13.1 time/y, p=0.027).

Comparison of people with hypertension according to their status of diagnosis and controlled by gender
Table 4 shows the results of the multiple logistic regression analysis of socio-demographic and clinical factors as well as health behaviors. Higher BMI was not associated with hypertension diagnosis (p=0.735) but was negatively associated with hypertension control (odds ratio [OR] 0.85 per 1 kg/m2, p=0.020) in men. However, in women, BMI was not associated with either diagnosis (p=0.727) or control (p=0.856) of hypertension. Higher education level (>6 years) was positively associated with hypertension control (OR, 5.23; p=0.013) only in women. A known diagnosis of diabetes was positively associated with hypertension diagnosis in men (OR, 4.26; p=0.014) but not in women (OR, 2.33; p=0.111). In contrast, having been diagnosed with diabetes was negatively associated with hypertension control in both genders, but the negative association was stronger in women (OR, 0.23; p<0.001) than in men (OR, 0.30; p=0.010). In women, frequent BP checkups (OR 1.06 per 1 time/y, p=0.011) and awareness of BP level (OR, 2.86; p=0.003) were positively associated with hypertension diagnosis, although they were not significantly associated with hypertension control. In men, awareness of BP level and number of BP checkups were not associated with either diagnosis (p=0.295 and p=0.192, respectively) or control (p=0.527 and p=0.187, respectively) of hypertension.
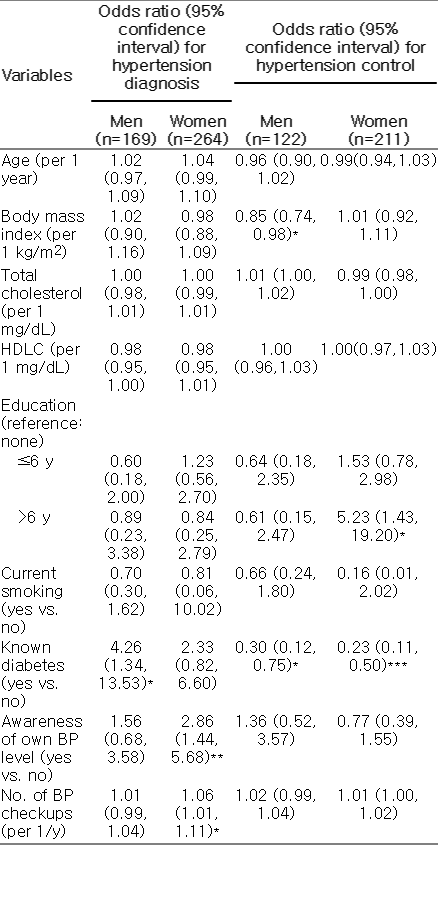
Factors associated with diagnosis and control of hypertension by gender
DISCUSSION
We investigated factors associated with hypertension diagnosis and control among community-dwelling older men and women. The overall prevalence of hypertension in the current study was 66.3%, which is similar to that of the 2012 KNHANES (64.7%) studies [6] . In our study, a total of 76.9% of hypertensive participants knew that they had hypertension, and 42.3% kept their BP controlled. Among the elderly subgroup (aged 65 years or older) of the 2008-2012 KNHANES, the hypertension awareness rate was 82.7% and the hypertension control rate was 54.4% [6]. There are a few possible explanations for the lower hypertension awareness and control rates in our study population. First, it has been reported that hypertension awareness and control are poorer among older people living in rural areas than those living in urban areas [24]. This regional difference might be associated with socio-economic status, health behaviors, and accessibility to health care services. Second, the KNHANES report defined controlled BP as SBP <140 mmHg and DBP <90 mmHg regardless of the presence of diabetes, while we used a lower cutoff (SBP/DBP <130/80 mmHg) for those with diabetes.
Hypertension diagnosis and control rates were not significantly different between older men and women in our study. However, we identified gender-specific socio-behavioral and clinical factors that contributed to the diagnosis and control of hypertension. Consistent with previous studies [4,25], sociobehavioral factors were significantly associated with hypertension diagnosis and control in women. The first step in changing one’s behavior to prevent or manage chronic disease is to be aware of one’s individual risk. Increased knowledge of CVD risk factors among women has been proven to influence them to take action to prevent CVD [26]. In a previous study, hypertension was the most frequently cited cause of CVD in Korean middle-aged women, and 67% of them reported knowing their own BP level [27]. In the current study, undiagnosed hypertensive women were less likely to know their BP level and check their BP. Only 49% of undiagnosed hypertensive women knew their BP level, whereas the rate was 72% among all hypertensive participants. Moreover, these women checked their BP eight times during the previous year, whereas average hypertensive patients checked their BP 19 times during the same period. Given these results, efforts to increase awareness of one’s own BP level through regular BP checkups may aid the prevention and management of hypertension in older women. Considering the gap between awareness of one’s own BP level and awareness of a desirable BP level [27], healthcare providers should provide counseling to improve hypertension awareness, especially in older women.
Our results also indicated that women with a higher education level were significantly more likely to have controlled BP than women with no education. Differences in socioeconomic status such as education, occupation, and income have been reported to be larger among women than among men [28]. These findings suggest that educational strategies can modify health behaviors more effectively among women. Recently, Cornwell and Waite [22] reported that interaction, information, emotional support, and social network resources may affect the risk of undiagnosed and uncontrolled hypertension. In our study population of older, community-dwelling Koreans, men and women are likely to have different roles and responsibilities in their families as well as in the community. Thus, older women have more limited social network resources, lower educational level, and higher caregiving responsibilities than men in the same community, which might lead to worse outcomes in the management of hypertension. Further studies are required to understand the relationship between hypertension control and community-based social networks to establish effective public health strategies to control hypertension among rapidly aging populations.
For BP control, clinical factors such as diabetes comorbidity, obesity, and blood cholesterol might have gender-specific relationships with hypertension diagnosis and control. Consistent with a previous study [4], diabetes was identified in this study as a common factor contributing to unfavorable BP control in both men and women. Diabetes and hypertension have a shared root in insulin resistance as well as a reciprocal relationship that leads to the vicious cycle between insulin resistance and endothelial dysfunction [29]. Insulin has a trivial net effect on BP regulation due to its multiple opposing hemodynamic actions of stimulating nitric oxide-dependent vasodilation and endothelin 1-induced vasoconstriction in healthy individuals [30]. However, insulin resistance caused by the hyperglycemic condition of diabetes breaks the balance between vasodilation and vasoconstriction by diminishing nitric oxide signaling in skeletal muscle arterioles, and this shift leads to a hypertensive response [31]. These pathophysiological links between hypertension and diabetes may create difficulties in maintaining optimal BP among hypertensive patients with diabetes. Animal models and observational studies in humans support the link between insulin resistance and endothelial dysfunction leading to CVD. Mice lacking insulin receptor substrate-1, which model type 2 diabetes, showed a hypertensive phenotype with impaired endothelium-dependent vascular relaxation [32]. Patients with both hypertension and type 2 diabetes have an approximately two-fold greater risk of CVD than non-diabetic patients with hypertension [33]. However, we cannot exclude the possibility that the lower control rate among hypertensive patients with diabetes in our analysis might be simply due to lower target BP levels for patients with diabetes (SBP <130 mmHg and DBP <80 mmHg). The Eighth Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 8) questioned whether a lower BP goal should be applied to hypertensive patients with type 2 diabetes due to a lack of evidence from randomized clinical trials, and recommended the same cutoffs for those with diabetes [34].
We also found that other factors were associated with hypertension control in each gender. In a study by Davarian et al. [35] that included 2634 Japanese adults aged 68 or older, a higher BMI was significantly associated with a higher SBP and DBP, but no gender-specific analysis was performed. In our study, the link between a higher BMI and uncontrolled hypertension was observed only in men. On the contrary, increased total cholesterol tended to be associated with uncontrolled hypertensive women, although this was not statistically significant. A previous study also suggested that hypertensive women tended to have more cardiovascular risk factors than men, such as central obesity, elevated total cholesterol, and low high-density lipoprotein [4], which might be caused by the physiological changes such as the abrupt drop of estrogen in postmenopausal women. Estrogen deficiency in postmenopausal women increases central adiposity and decreases muscle mass [36]. Although a strong relationship between hypertension and BMI exists, a well-known surrogate marker for general obesity has been established in the general population including older adults. In addition, a surrogate marker for central obesity such as waist circumference or waist to hip ratio, adjusted for BMI, should be considered in this population because BMI cannot completely capture the changes to body composition and fat distribution with aging, especially in older women.
The main strength of this study is that we used the KSHAP data, which included most of the population of older adults living in a rural community in South Korea. Resting BP was measured by a standard protocol throughout the study. These strengths might improve the ability of our study to represent community-dwelling older adults with hypertension, especially from a rural area of South Korea, and to add to our knowledge of hypertension control including the influence of behavioral and physical health factors. However, our study has several limitations. First, BP was measured at a single time point among all participants. Ambulatory BP monitoring and repeated measurements are recommended to assess diurnal and day-to-day BP variations and to exclude the influence of an observer bias and ‘white coat’ effect [37]. Thus, we cannot exclude the possibility of misclassification for the above reasons. Moreover, we were not able to collect detailed information on antihypertensive medication use, physical activity and diet, which also influence BP control. In future studies, more detailed data should be collected to comprehensively understand hypertension control among community-dwelling older adults.
Our study suggests that gender differences exist among factors associated with hypertension diagnosis and control in this population of community-dwelling, older adults. Hypertensive older adults with diabetes seem to be most susceptible to uncontrolled hypertension, regardless of gender. However, the impact of behavioral and cardiovascular risk factors on hypertension control might be different between men and women. Based on our results, gender-specific approaches are required to control hypertension effectively among older adults. Moreover, education-based health promotion strategies in hypertension control might be more effective in elderly women than in elderly men.
ACKNOWLEDGEMENTS
This study was supported by grants from the National Research Foundation of Korea (NRF-2011-330-B00137) and the Korean Health Technology R&D Project, Ministry of Health and Welfare, Republic of Korea (HI13C0715).
Notes
Conflict of Interest
The authors have no conflicts of interest with the material presented in this paper.