Psychological, Social, and Environmental Factors Associated With Utilization of Senior Centers Among Older Adults in Korea
Article information
Abstract
Objectives
The purpose of the study was to examine the relationships among the psychological, social, and environmental factors influencing the utilization of senior centers among older adults in Korea.
Methods
A questionnaire survey was administered to two types of older adults who lived in Seoul, Korea: 262 older adults who used senior centers (3 places) and 156 older adults who did not use senior centers.
Results
Our results showed clearly that the utilization of the senior centers in Korea is affected by higher self-efficacy (odds ratio [OR], 6.08; 95% confidence interval [CI], 3.31 to 12.32), higher perceived benefits (OR, 1.71; 95% CI, 1.16 to 4.36), lower perceived barriers (OR, 6.43; 95% CI, 3.07 to 11.45), higher family support (OR, 4.21; 95% CI, 2.02 to 8.77), and higher support from friends (OR, 4.08; 95% CI, 2.38 to 7.81). The results also showed that participants whose total travel time was 15 to 29 minutes (OR, 2.84; 95% CI, 1.21 to 3.64) or less than 14 minutes (OR, 4.68; 95% CI, 3.41 to 8.41) were more likely to use a senior center than those who had to travel more than 30 minutes.
Conclusions
This study showed that the utilization of senior centers in Korea is affected by psychological, social, and environmental factors, specifically by self-efficacy, perceived benefits, perceived barriers, social support, convenience of transportation, and total travel time to the senior centers. The effects of longer-term utilization of the senior centers by non-users on health-related outcomes in a large population warrant attention.
INTRODUCTION
The long-term care insurance system, one of Korea's most important health improvement services, was introduced in July 2008 [1]. This policy was developed primarily to promote the long-term health of the elderly through prevention [2]. Korea, like many developed countries with growing elderly populations, uses its senior centers as a means of promoting long-term health care and prevention. It was thought that prevention would lead to a reduction in national medical expenditures and the stabilization of fiscal insurance costs, while concomitantly improving the overall health and quality of life of senior citizens [3]. With the rapid growth of the aging population in Korea, it has been recommended that the government not invest in new and large infrastructure but to utilize existing senior centers for the implementation of the prevention of long-term care program. These senior centers provide not only social education, exercise, and recreation, but also preventive medical consultations and health promotion programs to enhance the quality of life of older adults [4]. Previous studies in advanced countries, including Korea, have suggested the positive effects of using the senior center on physical health (fall prevention, resistance exercise, and walking distance) [5-8] and psychological health (depressive symptoms, friendships, and stress-related distress) [9-11]. In spite of such proven effects both physically and psychologically, only 28.7% of older adults have ever used a senior center in Korea, and only 3.6% reported using the senior centers regularly [12]. In addition, the rate of using the senior centers in Korea is substantially lower than that in the United States (13.7%) [13].
In order to increase the proportion of users of senior centers, it is important to understand the health promotion behavior of older adults, and the complex behavioral process which affects choosing their health promotion behaviors [14,15]. Previous theories on what affects health promoting behaviors have focused on the cognitive factors of individuals [16]. However, the ecological perspective expands on the factors affecting human behavior to include social and environmental factors in addition to individual ones. From the ecological perspective on health promotion, health is a continuing interactive product of both the internal and external environments of individuals [17]. In particular, psychological, social, and environmental factors play the role of composing factors influencing the healthy lifestyle of the elderly, and explaining this relationship is important for building up an effective population strategy [18]. In this regard, the strategy should be implemented from multiple dimensions-it should be concerned not only with the personal level as a microscopic dimension but also the community/societal environment level as a macroscopic dimension. For reaching such a target, a multi-academic approach including social welfare should be taken in addition to health medication.
In Korea, mainly the socio-demographic factors and the status of use have been studied to increase the number of users of senior centers, but no multi-dimensional research on the psychological, social, and environmental factors affecting utilization of senior centers were found. It is necessary to understand the characteristics of the users by considering such factors and establishing an effective strategy of intervention with the senior center based upon such an understanding. The purpose of the study was to examine the relationships among the psychological, social, and environmental factors influencing the utilization of the senior center among older adults in Korea.
METHODS
Participants and Procedures
This study used a two-group cross-sectional comparative design. This study was conducted between March 2011 and April 2011 using a questionnaire survey to distinguish between two types of older adults who lived in Seoul, Korea. Three senior centers (i.e., Seodaemun-gu, Jung-gu, and Jongro-gu) were chosen among 30 senior centers in the metropolis of Seoul based on the population density using random sampling. One group consisted of 262 respondents (male 38.3%, female 61.7%, age 73.8±6.7 years, mean±SD) who used the senior centers (3 places) located in the metropolis of Seoul (i.e., Seodaemun-gu, Jung-gu, and Jongro-gu). Additionally, another group of 156 respondents (male 42.7%, female 57.3%, age 70.2±5.1 years) was generated of those who did not use the senior center by extracting subjects according to their sex and address by proportional stratified random sampling from the same neighborhoods of the Metropolis of Seoul. Furthermore, this study collected data face-to-face, and the six interviewers (five women, one man; professional interviewers of a research company) were carefully trained in an extensive didactic and experiential course in interviewing. Before collecting data, the interviewers were required to demonstrate a minimum at least two consecutive training interviews.
Users of the senior center were defined to be "patrons regularly using the facility two or more times a week" and non-users are "patrons irregularly using the facility less than once a week" or "those who had never used it" [19]. The purpose of the research and the content of the survey's questionnaire were fully explained to each participant before they gave written informed consent. This study was approved by the institutional review board of Waseda University.
Measures
Socio-demographic variables
Socio-demographic variables were obtained by questionnaire. Variables comprised gender, age, height, weight, education level, marital status, employment status, and present illness. There were three age demographics: 65 to 69, 70 to 74, and 75 and older [20]. Education level was divided into four levels: less than elementary school completion, attended middle school, attended high school, and at least some technical school or college [20]. Respondents were posed with a yes-or-no question used by the Ministry of Health and Welfare to determine their employment and marital status. Respondents were posed with a yes-or-no question used by the actual condition survey on older adults to determine their state of physical health: "Do you have any illness that has lasted over three months?" [20]. Height and weight were used to calculate the body mass index, and the results were classified into the standard two categories proposed by the World Health Organization: underweight or normal weight (24.9 or under), and overweight or obese (25.0 or more).
Psychological, social, and environmental variables
Psychological factors were self-efficacy, perceived benefits, and perceived barriers for the senior center, while the social factors were social support rendered to the senior center (i.e., family support and friend support). The self-efficacy scale was composed of six items that evaluated the prospects of continuous use despite perceived barriers of using the senior center (such as convenience of transportation, mental stress, no time, bad weather, etc.). The scale let the respondents select one of five questions from 1 (strongly disagree) to 5 (strongly agree). This scale was verified in its reliability (α=0.90) and construct validity (goodness of fit index [GFI]=0.98, adjusted goodness of fit index [AGFI]=0.95, root mean square error of approximation [RMSEA]=0.06).
The perceived benefits and perceived barriers belonging to the psychological factors of using the senior centers were composed of 8 and 6 items, respectively. The perceived benefits were to "aleviate stress and feel comfortable" and "maintain proper weight", while perceived barriers were "family does not recommend" and "no companion to go with". The scale let the respondents select one of five responses from 1 (strongly disagree) to 5 (strongly agree). The scale for the perceived benefits was verified for its reliability (α=0.84) and construct validity (GFI=0.96, AGFI=0.92, RMSEA=0.08), and the same of the perceived barriers was verified for its reliability (α=0.81) and construct validity (GFI=0.97, AGFI=0.94, RMSEA=0.06).
For the social support, 6 items were included to evaluate the support of family and friends, and the scale let the respondents select one of four responses from 1 (do so always) to 4 (never did so). This scale was verified in its reliability (α=0.89) and construct validity (GFI=0.98, AGFI=0.95, RMSEA=0.06).
For the environmental factors, the total travel time to the senior centers and convenience of transportation were investigated. The total travel time from the house to the senior center was written by hand by the respondents, and it was classified as a median value estimated from the data obtained to be in one of three categories: 1, more than 30 minutes; 2, between 15 and 29 minutes; 3, less than 14 minutes. As for the convenience of transportation, the scale allowed respondents to select one of four possible responses from 1 (very convenient) to 4 (inconvenient) for four questions on "convenient means of transportation from the house to the senior center."
The index of appropriateness occupied the value of 0 to 1 together with the GIF and AGFI using the following four measures: the GFI, AGFI, RMSEA, and Akaike information criterion (AIC), but if the value came closer to 1, it was regarded as a more appropritate model for appropriateness, and more than 0.9 was deemed to be the criteria for judgment. In addition, if the RMSEA came closer to 0, it was judged to be a good model, and the model selected was below 0.08. Furthermore, the factor analysis models requiring modification were compared using AIC between, before, and after the modification. Models with better appropriateness are shown by the lower value of the AIC. At the same time, because judgment on the appropriateness by the chi-squared test is pointed out to rely strongly on the number of cases, it was not applied to this study as an index. Because their appropriateness index is good, applying the models was subject to all the pass coefficients being significant by the Wald test.
Statistical analysis
A total of 430 respondents were initially included in the study, of which 262 were the users of senior centers and 168 were non-users. Among the 168 non-users, 12 respondents answered the questionnaire on the utilization of the senior centers. Therefore, the data of 418 respondents-that is, all except those 12, were used for the analysis (male 40.4%, female 59.6%, average age 72.6±5.7 years, mean±standard deviation [SD]). The status of using the senior center was divided into two groups, users and non-users, and each relationship among the socio-demographic variables, and the social, psychological, and environmental factors was analyzed by a chi-squared test. Also, in order to examine the relevant factors after the effects between the variables were adjusted, logistic regression was conducted to establish the status of using the senior center as a dependent variable. Finally, the self-efficacy, social support, perceived benefits, and perceived barriers were each split into a higher group and a lower group according to the median value. The alpha level was set at 0.05. The SPSS version 18.0 (SPSS Inc., Chicago, IL, USA) was utilized to compute the statistics.
RESULTS
The characteristics of the respondents are shown in Table 1. Their age was 72.6±5.7 years (the minimum age was 65 years and the maximum age was 95 years). Among the respondents, 87 (20.8%) had an education level of at least some college, which is higher than the general level of older adults in Korea, 348 (83.3%) respondents were retired, 254 respondents (60.8%) were married, and 256 respondents (61.2%) replied that they suffered from disease. Compared to all older adults of Korea, the variables confirmed to have a distribution of more than 10 point were educational level, employment status, and present illness, and the characteristic of the group considered was higher educational level, but those having jobs were different from typical older adults in Korea (Table 1).

Basic characteristics of respondents
Socio-demographic factors in relation to the utilization of the senior centers from a univariate analysis were age (χ2=9.6, p<0.01), educational level (χ2=32.8, p<0.001), and employment status (χ2=14.1, p<0.001). The outcomes related to psychological, social, and environmental factors were self-efficacy (χ2=119.1, p<0.001), perceived benefits (χ2=4.3, p<0.05), perceived barriers (χ2=92.2, p<0.001), social support (χ2=137.4, p<0.001), travel time to the senior centers (χ2=22.5, p<0.001), and the convenience of transportation (χ2=91.0, p<0.001) (Table 2).
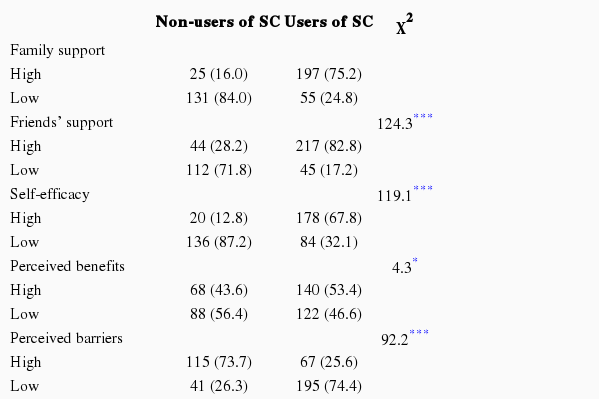
The relationship between psychological, social, and environmental factors on utilization of senior centers: univariate
Logistic regression was conducted to adjust for the effects between the variables and interpret them. Significant results were found in females (odds ratio [OR], 2.89; 95% confidence interval [CI], 1.76 to 4.47), those having middle school (OR, 3.33; 95% CI, 1.80 to 6.14) and high school education (OR, 5.66; 95% CI, 2.94 to 10.87) than those with an educational level of less than elementary school completion, jobless people (OR, 3.01; 95% CI, 1.65 to 5.46). Significant relationships were found in the following group of respondents: those of higher self-efficacy (OR, 6.08; 95% CI, 3.31 to 12.32), higher perceived benefits (OR, 1.71; 95% CI, 1.16 to 4.36), lower perceived barriers (OR, 6.43; 95% CI, 3.07 to 11.45), higher family support (OR, 4.21; 95% CI, 2.02 to 8.77), higher family support (OR, 4.08; 95% CI, 2.38 to 7.81), travel time of more than half an hour, 15 to 29 minutes (OR, 2.84; 95% CI, 1.21 to 3.64), less than 14 minutes (OR, 4.68; 95% CI, 3.41 to 8.41), those considering the transportation convenience to be favorable in general (OR, 2.80; 95% CI, 1.41 to 6.46), those considering it fair (OR, 3.71; 95% CI, 2.81 to 8.66) and very favorable (OR, 6.72; 95% CI, 3.14 to 14.71) (Table 3).

The relationship between psychological, social, and environmental factors on utilization of senior centers: multivariate analysis
DISCUSSION
This study examined the psychological, social and environmental factors associated with the utilization of senior centers. Our results showed that the utilization of the senior center in Korea is correlated with self-efficacy, perceived benefits, perceived barriers, social support, convenience of transportation, and total travel time to the senior center.
Among the psychological factors, users of senior centers were revealed by this study to have greater self-efficacy than non-users. Previous studies of older adults have reported that the higher the self-efficacy was, the more extensive their health behaviors were in relation to the relationship between health behavior and self-efficacy [21,22]. Such reports imply support for the theory that higher self-efficacy causes the execution of greater health behaviors, and also it indicates that the self-efficacy regarding the health behavior of Korean older adults is related to attending a senior center.
This study also found that use of the senior center was significantly correlated to both perceived benefits and barriers. Previous studies have reported that "the content of programs" provided by the senior center was a factor for non-use as one of the perceived barriers [23-26]. In addition, the assertion of "no time to go" was reported to be related to the utilization of the senior center [24]. This indicates that proper assistance to remove the perceived barriers is required for the purpose of leading the non-users to use the facility [25,26]. For instance, some of the methods we can consider to eliminate the perceived barriers are motivating seniors, providing various programs including health programs that are suitable for helping individuals maintain a healthy life, and guidance in using such programs.
Regarding social support, this study found that those who had a family that provides more social support used the senior center more regularly. Such findings suggest that older adults in Korea were influenced by family support, which is in line with previous studies from other countries [11,27]. As family social support for the elderly includes psychological and economic support, it is closely related to the support of the family. It should also be noted that the importance of social support from friends emphasizes the life pattern changes of the elderly and the changes in family style. Previous studies have also reported that the social support of friends affected the utilization of senior centers [28]. Additionally, the relevance of using the senior center by the elderly with or without a spouse was not found by this study, but the elderly living by themselves used the center less than did those with a spouse or family. This could be because older adults living alone are apt to be isolated from the surrounding environment and have fewer opportunities to obtain information and support from society, which restricts their participation within society [29]. Accordingly, an appropriate approach to the elderly living alone will help to enhance their utilization of senior centers.
Among environmental factors, use of senior centers is associated with environmental factors such as the total time they travel to the senior center, and the convenience of transportation means. Those who have a short travel distance from their home to the senior center use the facility more regularly, and this coincides with the result of the previous studies on the frequency and period of using the senior center [19,27]. A study on leisure activities and outings reported its relationship with the convenience of transportation [30]. Most of the long-term care prevention of long-term care facilities in Korea are situated in the convenient place. The elderly citizens' scope of activities is more limited than the young due to their poor health, and the weak, in particular, have difficulty in accessing senior center facilities, which makes it difficult for them to attend. In order to encourage senior center attendance, more convenient means of access such as shorter distance and better transportation should be taken into account. For example, transportation services for older people, or certain older people with physical limitations would be useful. Also, providing services for small local areas would be helpful.
There are some limitations to our study. Our study was a cross-sectional study and thus the cause-and-effect relationship between the utilization of the senior center and psychological, social, and environmental factors cannot be determined. For this, a longitudinal study or intervention study should be conducted to make such a relationship clear. Another weakness of the present study regards whether our findings can be generalized to the larger population. In our study, the users of the senior center had a higher educational background than that of non-users, and among the users of the senior centers, three percentage with a higher educational background was much higher than in the general Korean population.
This study indicates that such efforts to increase the rate of use as giving full consideration to the self-efficacy, perceived benefits and barriers, social support, total time, and convenience of access for aged citizens may be useful. This study is the first of its kind to describe the relevance between psychological, social, and environmental factors and utilization of senior centers. Our findings may contribute to the promotion of the prevention of long-term care program. In the future study, the effects of longer-term utilization of the senior center by non-users on psychological, social, and environmental factors in a large population warrant attention.
ACKNOWLEDGEMENTS
This study was supported by grants from the Waseda University Global COE Program "Sports Science for the Promotion of Active Life" (2010-2011).
Notes
The authors have no conflicts of interest with the material presented in this paper.