Overview of the Burden of Diseases in North Korea
Article information
Abstract
This article evaluates the overall current disease burden of North Korea through the recent databases of international organizations. It is notable that North Korea as a nation is exhibiting a relatively low burden from deaths and that there is greater burden from deaths caused by non-communicable diseases than from those caused by communicable diseases and malnutrition. However, the absolute magnitude of problems from communicable diseases like TB and from child malnutrition, which will increase the disease burden in the future, remains great. North Korea, which needs to handle both communicable and nutritional conditions, and non-communicable diseases, whose burden is ever more increasing in the nation, can now be understood as a country with the 'double-burden' of disease.
INTRODUCTION
A clear understanding of the health status and disease burden of North Korea is necessary for planning effective aid and for ensuring human security, the foundation of sound unification. However, it is difficult to see the whole picture of the situation in North Korea due to the lack of reliable data, and continuous controversy has surrounded this issue [1].
The health care situation in North Korea is usually assessed and estimated based on data from international organizations, non-governmental organizations, North Korean refugee studies, and press reports. Normally, it has been reported by international organizations and international community that communicable diseases, such as tuberculosis (TB) and malaria, and childhood malnutrition are the major health problems of North Korea, and reports so far have also pointed out the complete inability of the North Korean health care system to treat or control the nation's health problems [2-4].
Along the same lines, the media has placed its emphasis on reporting mass mortality or morbidity due to malnutrition or communicable diseases. As a result, it could be easily assumed that, from the general public knowledge shaped by reports with a focus on communicable diseases and malnutrition, North Korea would have both the worst health status and health care environment in the world, with the disease structure of a low income country.
In this article, this general understanding is to be challenged, and the disease burden and structure of North Korea will be evaluated and understood in a more objective and balanced way in order to grasp the true picture of the nation's health status.
DATA SOURCES AND ANALYSIS
Generally, "burden of disease" or "disease burden" refers to the negative impact on a society or a nation or world due to the mortality and morbidity of a specific disease, and it has recently often been quantified with certain metrics. In this article, the methodology for examining North Korea's burden of diseases is simple: data have been drawn from a literature review on the mortality and major health issues of North Korea recently reported in a quantitative manner by international organizations, which are thought to be relatively more reliable than other sources of data.
There are four health issues in this article, mortality, communicable diseases, non-communicable diseases (NCD), and child nutrition conditions, and the basic sources of information on these issues was drawn from data reported recently by the World Health Organization (WHO) and United Nations Children's Fund (UNICEF), which are actively running several health programs in North Korea. To investigate the mortality of North Korea, data on mortality rates presented in the Global Health Observatory constructed by the WHO worldwide with the reference year of 2008 were utilized [5]. Using this data, the crude and age-adjusted death rate, mortalities according to age groups, and the structure of causes of death in North Korea were studied. The evaluation of communicable diseases was focused on TB and malaria, which have been recognized as the biggest health issues in North Korea and accordingly received the largest proportion of health care aid. The data from the World Tuberculosis Control [6] and World Malaria Report [7] published by the WHO in 2012 were utilized. For the issues with NCD, Noncommunicable Diseases in the South-East Asia Region [8] published by the WHO was used as a foundation. Finally, the present article bases its analysis on the childhood nutrition section of the Multiple Indicator Cluster Survey, a nationwide survey evaluated to have among the most reliable data, undertaken by UNICEF and the WHO in 2009 [9].
The basic data mentioned above were reorganized and reconstructed to analyze mortality levels and the disease structure by comparing North Korea to the world as a whole, South Korea, and the South-East Asian Region (SEAR), a WHO subregion mainly consisting of countries with low income and health status, of which North Korea is a member state. Through the comparison with other groups and referring to other various published data, the relative level of the disease burden of North Korea was studied.
MORTALITY AND CAUSES OF DEATH
The age-standardized death rate of North Korea was 858 out of 100 000. This value was higher than South Korea's 436 or China's 731, but it was lower than those of fellow SEAR countries like India's 1147 and Indonesia's 961 and around the same level as Egypt's 860 and Jordan's 873, which have been reported to be countries with relatively higher income levels than North Korea. Globally, the age-standardized death rate of North Korea ranked in the middle among all of the WHO member states and was the second lowest in the SEAR countries following that of Maldives.
When the crude death rates are categorized into three age groups (under 15, between 15 and 19, and over 60) and analyzed, the result shows that North Korea had lower rates in all three groups compared to the level of the world and SEAR (Table 1). The age group under 15 including children, in particular, had a lower death rate, at 244 out of 100 000, which is only half of the world level at 519 and SEAR's 515. The same finding could be evidenced by the comparison of other child mortality indicators. For instance, the infant mortality and under five mortality rates of North Korea were 26 and 33 out of 1000 live births, which are again only half of the world's average at 61 and 51, and SEAR at 77 and 55, respectively [10]. It seems clear that there have been huge improvements in the child death rate in North Korea as the values of the two child health indicators were 42 and 58, respectively, in 1995 which was during the 'March of Hardship'.
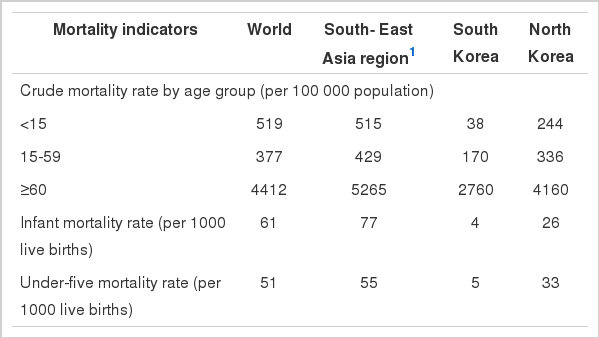
Selected mortality rates in North Korea and comparison groups for the year 2008
In Table 2, the structure of North Korea's causes of death was compared to the world level and that of high-income countries, low-income countries, and SEAR countries, based on the analysis of the reconstructed data on the causes of death. Globally, the NCD accounted for two-thirds of the total deaths, while communicable diseases and malnutrition took up only 25%. However, for low-income countries, communicable diseases and malnutrition were the leading causes of death. Although North Korea is classified as a low-income country, the structure of the nation's causes of death is unlike that of low-income countries; instead, it is closer to the worldwide level as NCD accounted for two-thirds of the total deaths. Cardiovascular disease (CVD) as a single disease group was the largest cause of death in North Korea, with an age-standardized death rate of 345 out of 100 000, which is two times higher than South Korea's 168 [11]. Communicable diseases and malnutrition, on the other hand, were responsible for 29% of the total deaths in North Korea. This figure was higher than those of high-income countries and South Korea, but it was only half that of low-income countries' 57%. Furthermore, the crude death rate due to communicable diseases and malnutrition was significantly lower at only 251 out of 100 000, compared to African regions at 817, and slightly lower than SEAR at 286.

Proportion of deaths due to three categories of cause in North Korea and comparison groups for the year 2008
The analysis of the mortality and causes of death discussed above could lead to the interpretation that the burden of mortality due to communicable diseases and malnutrition in North Korea is relatively low in terms of both quantity, expressed in the death rate, and quality, represented by the structure of the causes of death. Therefore, North Korea should not be considered a typical low-income country with the death structure centered around communicable diseases.
BURDEN OF COMMUNICABLE DISEASE
The TB mortality rates have declined continuously in the past 15 years in North Korea, now to the level of only a small difference when compared to those of South Korea (Table 3). Those estimates, in fact, are shown to be considerably lower than the average values worldwide and those of SEAR. On the other hand, the current prevalence and incidence of TB in North Korea, which are 422 and 345, respectively, out of 100 000 population for the year 2011, are almost three times larger than South Korea's 149 and 100, and also much higher than those of SEAR, the region that has the highest incidence in the world.

Trends in the disease burden of tuberculosis in North Korea and comparison groups over the period 1995 to 2011
This phenomenon, in which the death rate and prevalence are decreasing while the incidence remains unchanged at a high level, could be interpreted as that the number of patients receiving the proper treatment is steadily increasing, and treatment success rate is maintained at a high level [12]. However, the fact that the absolute rates of prevalence and incidence are high reflects that the amount of aid provided is insufficient for the magnitude of the crisis, and the disease continues to be spread [13]. In conclusion, North Korea can still be considered to be a country with a relatively high burden of TB even though the absolute disease burden from TB has been decreasing in terms of a continuous decline in the death rate and prevalence [14].
Malaria, another communicable disease now of less importance in North Korea, ravaged the nation from the mid-1990s to the early 2000s, and an outbreak in 2000 resulted in over 200 000 cases. However, the total number of patients has been decreasing at a steady rate; in addition, the incidence is reported to have dropped to around 10 000 per year since 2005. The current incidence of malaria in North Korea is found to be one of the lower ones in Southeast Asia, and the nation has currently been ranked at a pre-elimination stage for malaria.
Communicable diseases other than TB and malaria are also causing problems. Infections that cause pneumonia and diarrhea are the leading causes of child death, and it has been reported that over one third of the school-age children in North Korea have diseases caused by intestinal parasites [15,16]. Furthermore, North Korea is expected to have a significant incidence of hepatitis B and sexually-transmitted infections [17]. Meanwhile, North Korea reports that its vaccination rate for essential communicable diseases has reached the level of the developed countries. Whether the cold chain, which determines the efficacy of vaccines, is operating under normal conditions is, however, still questionable [18,19].
In summing up this section, it could be understood that communicable diseases are the area where most international attention and aid have been directed, and improvements in most of their aspects have been made. Despite such progress, the high burden of TB North Korea is still facing and other communicable diseases that have received relatively less attention and whose status cannot be fully grasped, continue to make the burden of communicable disease on the nation heavy and threatening.
BURDEN OF NON-COMMUNICABLE DISEASE
Developing countries in recent days are experiencing 'double burdens' of disease in that the burden of NCD is increasing in parallel with the previously existing health problems of communicable disease and malnutrition. North Korea as a nation seems not to be an exception. The disease group of the highest burden in North Korea, estimated by WHO's Global Burden of Disease study in 2004, was, surprisingly, CVD-about three times higher than that of South Korea [20].
The recent NCD status report on the SEAR countries also points to the relatively heavy NCD burden of North Korea [8]. For example, North Korea has been found to have the highest death rate from CVD in this region. Furthermore, factors that affect a nation's NCD burden-both on the society and the individual levels-are found to work in the direction of increasing the weight of the NCD burden in North Korea (Figure 1). As for societal factors, North Korea has the highest urbanization rates and the highest population proportion of the elderly among SEAR countries, not to mention that the nation was already classified as an aging society in 2006. On the individual level, the rates of risky behaviors, such as tobacco use and unhealthy use of alcohol, were observed to be the highest in the same WHO subregion as well. Based on all this, it could be concluded that North Korea had met the criteria for an increased NCD burden even before the time of economic hardship in the mid- to late-1990s. Therefore, it can be concluded that the current NCD-centered death structure of North Korea has resulted mainly from the accumulated NCD burden before the economic hardship and the hardship seemed to have accelerated the burden that already existed.

Following this line of argument, the generation who spent their infancy and developmental phase in the time of economic hardship would be of particular interest in terms of assessing future health problems. This specific group of people, who experienced malnutrition in their infancy and/or developmental phase, already exhibits a significant difference in height when compared to the comparative group of South Korean adolescents [21]. Based on the Thrift Phenotype Hypothesis, which suggests that such groups of people-those malnourished in their infancy or developmental phase-are more vulnerable to NCD incidence as they age, the future burden of NCD in North Korea will increase [22].
It is also important to be aware that the total disease burden of NCD is definitely greater than what could be estimated from the causes of death analysis alone. The reason is that NCD could induce significant loss in quality of life due to disability. When considering the total burden of NCD from premature deaths and survivors' poor quality of life, therefore, NCD causes, without a doubt, the largest disease burden in North Korea. Establishment of this understanding is important in the accurate assessment of the disease burden of North Korea, and recently the WHO has also been emphasizing the importance of this point [17].
BURDEN OF CHILDHOOD MALNUTRITION
As the media and non-governmental organizations have reported that several hundred thousands of children died from starvation during the period of economic hardship, the nutritional deficiency of North Korean children is an issue that has received worldwide attention [23].
In North Korea, 32% of children under the age of 5 were stunted (chronic malnutrition), and the severity of this health condition is greater for older ages, as around half of the children over the age 4 were in this group. In addition, 19%, or 1 out of 5 children, were underweight for their age. These outcomes were worse than the global averages for stunting and underweight, 26% and 16%, respectively (Table 4). In fact, the data for North Korea are closer to those of the African countries known to suffer from the most severe childhood malnutrition in the world, with 36% and 18% for stunting and underweight, respectively, signifying the gravity of childhood malnutrition as a health problem [24].

Nutritional status of children under five in North Korea by province for the year 2009
What further complicates the problem is that there exists a huge regional disparity in childhood malnutrition. The five provinces located in the northeast area, Ryanggang, North Hamgyong, South Hamgyong, Kangwon, and Jagang, exhibited significantly higher rates of children with stunting and underweight than other regions. The rates of stunted and underweight children in Ryanggang, specifically, were 45% and 25%, respectively, and these estimates were higher than the rates of the Sub-Saharan region known for the most serious childhood malnutrition in the world, at 40% and 21%, respectively.
Pyongyang, on the other hand, recorded about half the estimates of the stunting and malnutrition rates for Ryanggang. Such regional differences in child malnutrition status are apparently due to the differences in food security among different regions [25]. Mountainous areas, such as Jagang, Ryanggang and North Hamgyong, are known to be most vulnerable to food security issues. In other words, these provinces benefit relatively less from international food aid.
From the fact that half of the children under age 5 in North Korea live in those regions [26] and child malnutrition increases vulnerability to almost all diseases, the burden of disease that would be experienced in the future by the malnourished children of such areas will be immense. For both humanitarian and public health reasons, the current childhood nutrition gap based on geographical region must be reduced and, eventually, eliminated.
CONCLUSION
In this article, an effort to understand the current disease burden of North Korea is made on the basis of the analysis of the databases provided by international organizations. The biggest obstacle for understanding the accurate health status of North Korea, needless to say, is the lack of the validity and reliability of its data, and the problem of data quality is thus reflected in the present article as well. In particular, questions can be raised regarding the credibility of data on causes of death since the WHO ranked the evidence power of North Korea's raw data as the lowest level. In spite of this inherent limitation, it is concluded that to the extent we can have an understanding of the latest and most comprehensive health situation of North Korea, it is possible only through international agencies conducting health programs and communicating with North Korea and its people.
It is worth noting that North Korea as a nation is exhibiting a relatively low burden from deaths, including those of children, and that there is a greater burden from deaths caused by NCD than from those caused by communicable diseases and malnutrition. However, the absolute magnitude of problems from communicable diseases like TB and from child malnutrition, which will increase the disease burden in the future, remains great. Therefore, North Korea, which needs to handle both communicable and nutritional conditions, the primary factors of the disease burden in low-income countries, and NCD, the main part of the disease burden in developing countries, whose burden continues to increase in the nation, can now be understood as a country with the 'double-burden' of disease.
The huge health disparity between North and South Korea, needless to say, could greatly impede safe and stable unification and human security establishment. In order to reduce the health gap, aid for North Korea should be planned with such a strategy that would alleviate the current disease burden of the nation and minimize the disease burden of the reunified Korea as a whole. The blueprint for this strategic plan could only be possible with the balanced understanding of the disease burden and structure of North Korea.
Notes
The authors have no conflicts of interest with the material presented in this paper.