Empowering Rural Housewives in Iran: Utilizing the Transtheoretical Model to Increase Physical Activity
Article information

Abstract
Objectives:
Rural housewives are integral to household management and family care, yet their sedentary lifestyles present significant health risks. This study used the transtheoretical model (TTM) to investigate strategies that encourage and maintain regular exercise habits among rural housewives.
Methods:
A semi-experimental study was conducted in 2021 with 114 housewives aged 30 to 59 who attended rural health centers in Gorgan, Iran. Participants were randomly assigned to 1 of 2 groups. Data collection involved a validated questionnaire that gathered demographic information and constructs of the TTM. The intervention group participated in a comprehensive educational program, which included four 60-minute sessions. Data were collected again 6 months post-intervention and analyzed using descriptive and inferential statistics in SPSS version 21.
Results:
The study encompassed women with an average age of 39.75±6.05 years, the majority of whom had educational levels below a diploma, and over 90% were married. We observed strong correlations between the processes of change, self-efficacy, and decisional balance. At the outset, there were no significant differences in demographics or model structures between the 2 groups. However, 6 months post-intervention, the intervention group exhibited statistically significant differences in the mean scores of model structures, stages of change, and body mass index (p<0.05).
Conclusions:
This study highlights the importance of physical activity training for rural housewives. The findings suggest that the educational intervention, which utilized the TTM, significantly impacted the participants’ model structures and their stages of change.
INTRODUCTION
Insufficient physical activity (PA) represents a significant global public health concern associated with a range of health issues [1,2], including chronic diseases such as heart disease, diabetes, and obesity [3]. For housewives, inactivity can pose a health risk by encouraging a sedentary lifestyle and increasing the likelihood of developing these conditions [4].
Housewives frequently struggle to find time for physical exercise amidst their household responsibilities. Research has consistently demonstrated that housewives exhibit lower levels of PA [5]. This trend is not unique to any specific region; in Iran, for example, studies have similarly revealed that PA among housewives is markedly low [6].
Regular PA can help prevent chronic diseases, improve cardiovascular health, increase strength and flexibility, ameliorate body composition, reduce the risk of osteoporosis, improve pregnancy outcomes, and contribute to overall well-being in housewives [7-9]. However, rural housewives face various challenges in maintaining a consistent physical exercise routine, including limited availability of facilities, lack of social support, and cultural norms [4,10]. Strategies to increase PA among rural women may include educating them about the benefits of physical exercise, promoting self-efficacy through setting achievable goals and providing support and positive feedback, addressing barriers to PA, creating opportunities for group exercise, and incorporating enjoyable activities [11,12].
Education is a powerful tool for improving health behaviors, including participation in PA [13,14]. The transtheoretical model (TTM) provides a comprehensive framework for understanding behavioral changes, encompassing stages of change, processes of change, and decisional balance. Additionally, TTM emphasizes the importance of self-efficacy and social support, which are essential factors in facilitating behavioral modifications [15,16].
The TTM comprises various components, including stages of change, processes of change, and decisional balance. The stages of change are sequential phases—pre-contemplation, contemplation, preparation, action, and maintenance—that individuals experience as they progress toward altering their behavior. Processes of change refer to cognitive and behavioral strategies used to navigate the stages of change, such as self-reevaluation, self-liberation, and reinforcement management. Decisional balance involves weighing the advantages and disadvantages of behavior modification, aiding individuals in making informed choices about changing their behavior [17]. Research specifically addressing rural housewives is scarce, despite the possibility that they encounter distinct obstacles to PA. Although some studies have suggested that TTM-based interventions can effectively change PA behavior, the evidence is mixed, and there is a lack of research on particular intervention strategies. These deficiencies underscore the need for more comprehensive research on the efficacy of TTMbased PA interventions for rural housewives [18,19]. An educational intervention based on the TTM is anticipated to offer numerous benefits for rural housewives. These benefits include increased awareness and knowledge, enhanced motivation for change, improved self-efficacy, behavior modification, and promotion of physical and mental well-being, as well as social and community support.
An intervention was designed to empower rural housewives, helping them to adopt and maintain regular PA, which can positively impact their health and overall quality of life. To our knowledge, no studies have yet evaluated the effectiveness of the TTM in promoting PA among rural housewives. This study aimed to assess the impact of a TTM-based educational intervention on Iranian rural housewives.
METHODS
From June 31, 2020 to January 15, 2021, a semi-experimental study was carried out in a northern region of Iran, focusing specifically on housewives residing in a village setting.
Sampling Method and Sample Size
To mitigate the confounding effects of economic, cultural, and social factors on women’s knowledge, attitudes, and practices regarding PA, a systematic sampling method was utilized. Initially, 24 comprehensive rural health service centers were divided into 3 regions based on their geographical locations: north, south, and center of the city. Subsequently, using a block randomization approach, 6 health houses were selected from each region. From these, 2 blocks were chosen at random, with 1 designated as the control group and 1 as the intervention group. Each group comprised 57 women who sought services at the health centers.
To select eligible participants, we extracted a list of all middle-aged women who met the study criteria from the selected health centers. This list was sorted in non-descending order, and samples were chosen through systematic sampling by determining the sampling interval (k=N/n). This method was intended to ensure that the sample was representative of the broader population and to minimize the impact of confounding variables.
Based on a previous study, and using average values and standard deviation at a confidence level of 0.99 and a statistical power of 80%, the sample size was calculated to be 52 individuals using a specific formula [20]. To accommodate a potential drop-out rate of 10%, the sample size was increased to 57 individuals per group. Consequently, the total number of participants in the study was determined to be 114 individuals. A tailored behavior intervention, with a minimum duration of six months, was identified as the most appropriate approach [21]. Following a 6-month follow-up period, two women from the intervention group were excluded from the study due to pregnancy. In the control group, 2 women were excluded because they moved to the city, and 1 woman was excluded due to pregnancy. Figure 1 presents a flowchart illustrating the steps of the study.
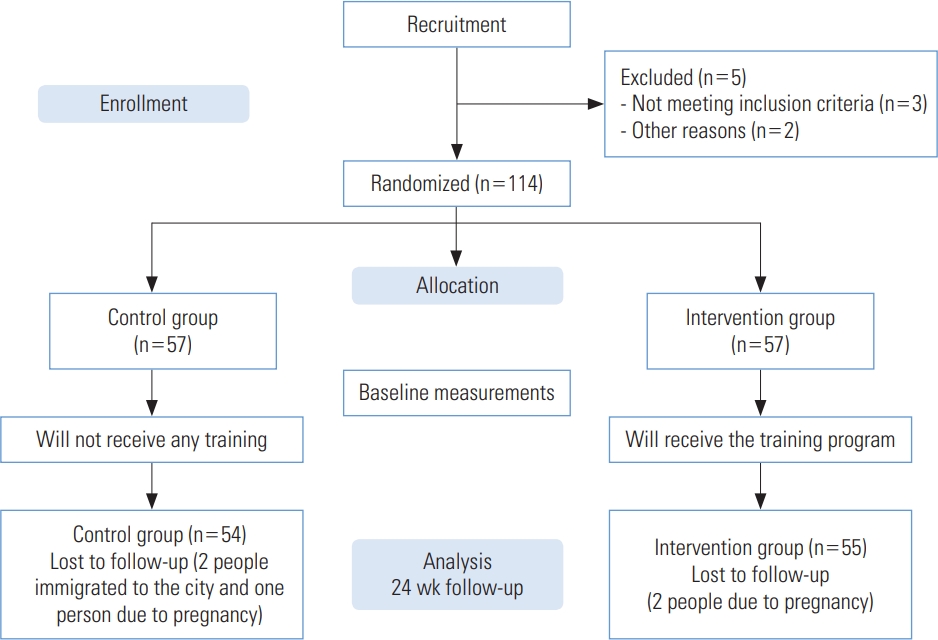
Flowchart of the intervention process.
Eligibility Criteria
The inclusion criteria for the study were as follows: residency in the selected villages, literacy, an age range of 30 years to 59 years, women gender, willingness to participate in the project, non-pregnancy, and the absence of physical or motor limitations.
Intervention
The intervention utilized the TTM as its theoretical framework. During the initial session, the purpose of the study and its significance for women were clearly outlined. The educational content included interactive in-person activities such as brainstorming, group meetings, and skills training. Additionally, part of the content was disseminated through a dedicated group on an Iranian social network. At the end of each training session, participants received pamphlets and training booklets.
Women were classified into separate groups based on an initial assessment of their stage of change, which resulted in five groups: pre-contemplation, contemplation, preparation, action, and maintenance. Each group received a tailored set of educational programs, interventions, and strategies. The sessions typically lasted 60 minutes, and meeting times were scheduled in coordination with the women’s preferred hours.
Individuals in the pre-contemplation and contemplation stages were encouraged to become more aware of PA through the provision of information and education, as well as by highlighting the benefits of an active lifestyle and the risks associated with sedentariness. The goal was to improve their understanding and acknowledgment of the significance of regular PA. Women in the preparation phase were provided with a daily activity schedule and guidance on setting goals. They were also urged to commit to regular PA. For those in the action and maintenance phases, a variety of PA types were introduced, including warm-up, endurance, flexibility, balance, and strength exercises, as well as isometric workouts. These were demonstrated using visual aids and educational videos shared on social media platforms. Additionally, techniques such as deep breathing, muscle relaxation, and meditation were taught. To promote adherence to the exercise regimen and manage external factors, reminder messages were sent out.
During the study, we leveraged the capacities of local officials, particularly the village council. We held training sessions with council members to facilitate coordination and create a supportive environment for women’s PA in the village. To raise awareness, we installed educational banners throughout the area. In light of the lack of a suitable gym or park, the village council arranged sports competitions to motivate women, nurture their competitive spirit, and boost their self-efficacy. The control group did not participate in these training sessions during the intervention period. However, they did receive a training session afterward, which included video clips and educational image presentations. Table 1 presents the educational program implemented for the intervention group.
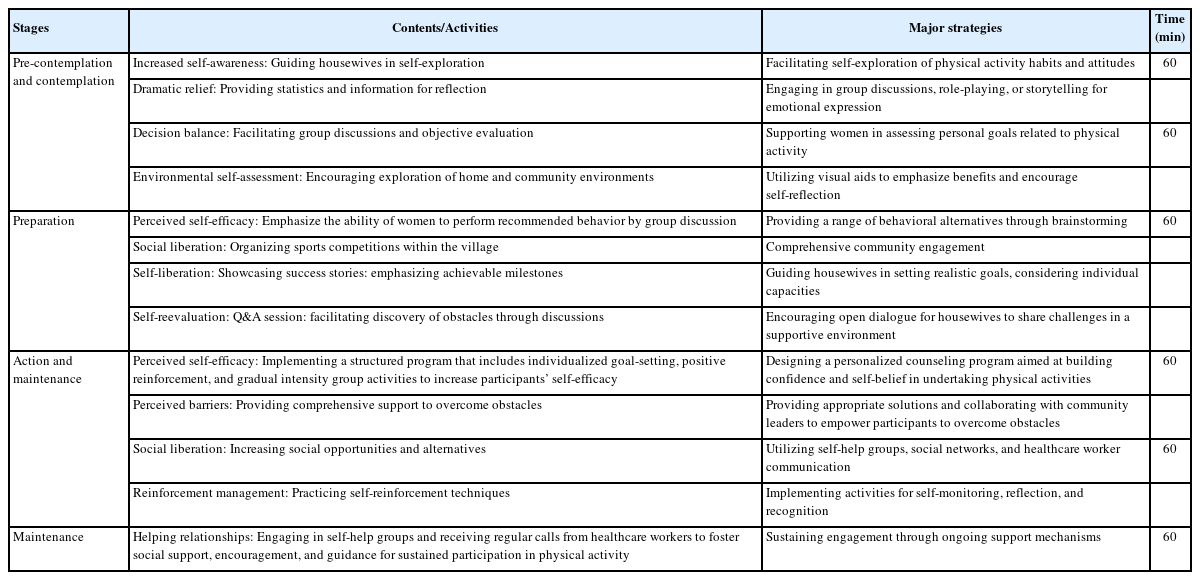
Educational program implemented for the intervention group
Instruments and Measures
The data collection tool used in this study was a standardized questionnaire designed around the constructs of the TTM. Readiness for change, decisional balance, and self-efficacy are key factors that collectively influence the processes of change. Decisional balance, which involves weighing the pros and cons of change, has been identified as a significant predictor of an individual’s readiness for change. Additionally, self-efficacy, which refers to one’s confidence in their ability to successfully implement change, plays a vital role in facilitating changes in work processes. The relationship between decisional balance and the stages of change has been further explored, with findings indicating that decisional balance acts as a mediator that affects progression through the stages of change [22].
The validity and reliability of the questionnaire were previously established by Mohammadi and Mehri [23] through a review by an expert panel. Cronbach’s alpha, a widely used measure for assessing internal consistency in research, is generally expected to be at least 0.7 to support the null hypothesis. However, it is important to consider the effects of inconsistent response patterns and the number of scale items on the degree of consistency. In this study, which had a sample size of 30, Cronbach’s alpha indicated a high level of internal consistency for the instrument being assessed, with values ranging from 0.83 to 0.95.
The questionnaire was divided into 3 sections. The first section gathered demographic information, such as age, marital status, educational level, height, and weight. The second section was dedicated to assessing the stages of change. In the third section, self-efficacy was evaluated using a 10-question subscale. Additionally, the questionnaire featured 28 items designed to measure change processes, both behavioral and cognitive, on a scale that ranged from “not at all” (1 point) to “rarely” (2 points), “sometimes” (3 points), and “always” (4 points). The questionnaire also included a decision-making balance component, which consisted of 43 Likert scale items scored from “completely against” (1 point) to “against” (2 points), “agree” (3 points), and “completely agree” (4 points).
Data Collection
Questionnaires were completed through self-reporting by two groups before the educational intervention. The researcher explained the study’s purpose and the questionnaire’s structure before participants completed it. While the questionnaire was being filled out, the researcher remained available to offer guidance should any issues arise. Six months later, data were collected once more from both groups.
Statistical Analysis
Continuous variables were presented as the mean±standard error, and categorical data were expressed as the count and percentage (%). We assessed the normality of the data through graphical examination and by applying the Kolmogorov-Smirnov test. Demographic variables between the two groups were compared using the chi-square test and analysis of variance. We evaluated the relationship between the constructs of the TTM using Pearson correlation coefficients. Additionally, we compared the average TTM constructs between the two groups using the independent samples t-test. The threshold for statistical significance was set at p-value <0.05. All data analyses were conducted using SPSS version 21.0 (IBM Corp., Armonk, NY, USA).
Ethics Statement
The current study has obtained ethical approval from the Research Council of Golestan University under the reference No. IR.GOUMS.REC.1400.170. A written informed consent form completed by all study participants.
RESULTS
The average age of the women was 39.75±6.05 years, and more than half had educational attainment below the diploma level. Before the educational intervention, 90.3% of the participants were married. Demographic variables showed no significant statistical differences between the two groups (Table 2). Strong correlations were found between self-efficacy (r=0.526; p<0.001) and decisional balance (r=0.430; p<0.05) with the processes of change.
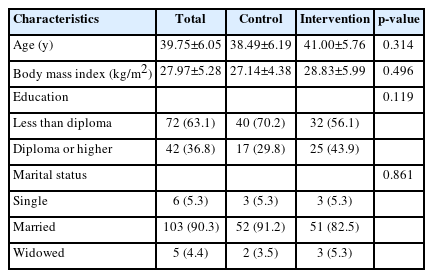
Demographic characteristics
Figure 2 illustrates the impact of the educational intervention, showing a shift in the participants’ stages of change. After the intervention, only a few women remained in the precontemplation stage, with the majority advancing to subsequent stages of change.
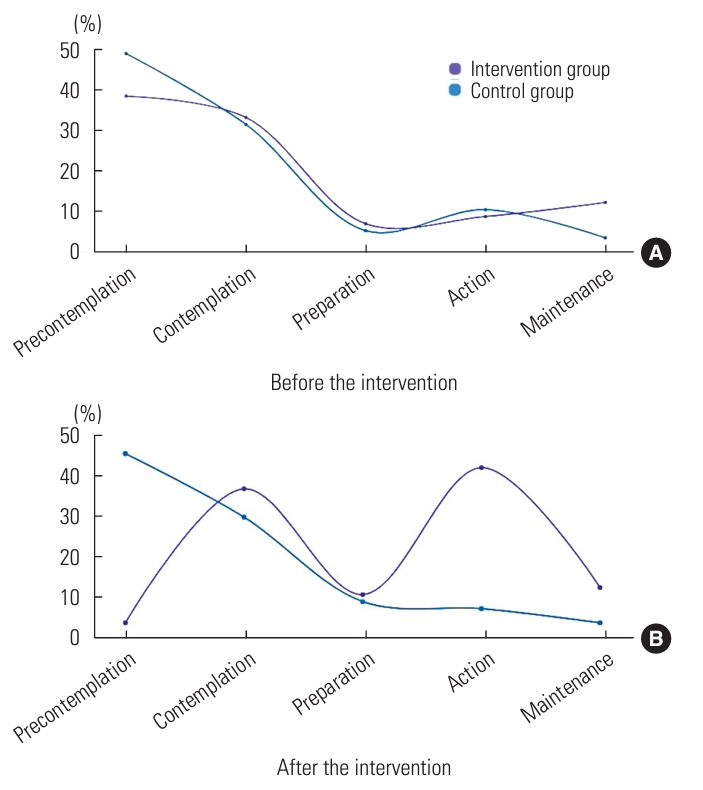
Comparison of stages-of-change percentages between the control and intervention groups (A) before and (B) after.
According to Table 3, the results of the independent t-test indicated that, following the educational intervention, the participants in the intervention group achieved higher average scores in the model constructs than those in the control group. Additionally, there was a significant decrease in the average body mass index (BMI) in the intervention group after the intervention.
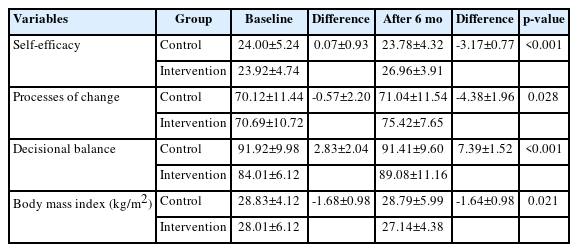
Changes in the control and intervention group after 6 months
DISCUSSION
PA training is crucial for maintaining good health and well-being for all individuals, including housewives. Housewives may lead sedentary lifestyles because of their domestic duties, potentially resulting in health problems such as obesity, heart disease, and diabetes [24]. The study’s findings emphasized the significant effect of the educational intervention on the intervention group compared to the control group, with respect to the average scores of the model constructs, stages of change, and BMI.
In our study, after the educational intervention, the intervention group showed a statistically significant reduction in BMI compared to the control group. A systematic review and meta-analysis reported on the effectiveness of PA interventions in reducing individuals’ BMI [25]. The notable decrease in BMI among housewives in the intervention group following the educational intervention on PA can be ascribed to the synergistic impact of heightened awareness, improved knowledge, and the adoption of healthier lifestyle practices promoted by the intervention.
Our study findings indicate a robust association between change procedures and both perceived self-efficacy and decisional balance. This suggests that individuals with higher self-efficacy and a balanced approach to decision-making are more inclined to enact positive changes and progress through the different stages of the change model. Put simply, individuals who are confident in their ability to start and sustain their chosen behavioral changes, and who approach decision-making with equilibrium, are more apt to successfully move from one stage to the next in the process of change. These findings align with those from previous research [26,27].
In this study, we noted significant differences between the intervention group and the control group regarding the stages of change. Specifically, participants in the intervention group demonstrated a marked shift from the precontemplation stage to the contemplation stage, with a greater number advancing to the action stage compared to those in the control group after a 6-month intervention period. The stages of change reflect the various psychological states that individuals experience during the process of behavioral change [18]. Similar shifts toward more advanced stages of change have been observed in other studies employing the TTM [28,29].
The results of our study showed a significant difference in the average scores of the model constructs between the intervention group and the control group 6 months following the educational intervention [30,31]. This underscores the success of the intervention in improving participants’ understanding and application of the model constructs. Research indicates that educational interventions grounded in the TTM are especially effective when they are tailored to an individual’s particular stage of change and behavior [18]. In our study, participants in the intervention group were categorized according to their stages of change, enabling personalized and targeted educational interventions that met the distinct needs of each subgroup.
The study focused on promoting PA among rural housewives, highlighting the importance of addressing their unique needs and leveraging the capacity of village councils to create a supportive environment. The individualized approach tailors the intervention based on each woman’s stage of change relative to the educational content, thereby increasing the intervention’s effectiveness and relevance and empowering rural housewives to improve their overall well-being. A limitation of the present study was the absence of behavioral monitoring and reliance solely on self-report data. Future research should consider incorporating objective measurements of behavior and include diverse age groups in the village setting to enhance the generalizability of the findings.
This study highlights the importance of aerobic exercise training tailored specifically for housewives in rural areas. The educational intervention, which combined in-person and online instruction based on the TTM, significantly impacted the participants’ model structures and stages of change. For example, participants reported increased motivation to exercise and improved physical fitness. These results underscore the necessity of implementing targeted PA programs for rural housewives to promote their well-being and encourage a more active lifestyle.
Notes
Conflict of Interest
The authors have no conflicts of interest associated with the material presented in this paper.
Funding
None.
Author Contributions
Conceptualization: Borhani M, Hosseini ZS. Data curation: Borhani M, Shahabodin N, Kiani M. Formal analysis: Hosseini ZS, Mehri A. Funding acquisition: None. Methodology: Borhani M, Hosseini ZS, Abedi M. Project administration: Borhani M. Visualization: Hosseini ZS. Writing – original draft: Hosseini ZS, Kiani M, Shahabodin N. Writing – review & editing: Hosseini ZS, Borhani M, Mehri A, Abedi M.
Acknowledgements
The authors express their gratitude to the village housewives for their enthusiastic involvement in the research, and they acknowledge and value the support and cooperation of the village officials.