Association Between Tobacco Smoking and Dental Caries in the Indonesian Population: Results of a National Study in 2018
Article information

Abstract
Objectives
The 2018 Basic Health Research (RISKESDAS), conducted by the Ministry of Health of the Republic of Indonesia showed a high prevalence of dental caries (88.8%) in Indonesia and suggested that smoking tobacco was associated with an increased risk of dental caries. This study analyzed the association between tobacco smoking and dental caries in the Indonesian population.
Methods
This was a cross-sectional analysis of secondary data collected from RISKESDAS 2018. The study population included 35 391 Indonesians aged ≥10 years from all 34 provinces. The decayed, missing, and filled teeth (DMFT) index was used to measure dental caries. Smoking status was assessed qualitatively based on smoking activity, and the level of smoking exposure was assessed based on the Brinkman index. A multivariable logistic regression analysis was employed to examine the relationships of smoking status and smoking exposure levels with the DMFT index.
Results
Of the population aged ≥10 years, 36% had a DMFT≥8 (females: 37.5%, males: 33.9%). Almost one-fourth (23.4%) were current smokers, and 4.1% were ex-smokers. Furthermore, 26.4% had a Brinkman index ≥400, indicating heavy smoking. According to the multivariate analysis, current smoking status was associated with the risk of DMFT≥8 in males (adjusted odds ratio [aOR], 1.40; 95% CI, 1.27 to 1.55; p<0.001) and overall (aOR, 1.07; 95% CI, 1.00 to 1.14; p=0.037). In females, ex-smoking was associated with a 41% higher risk of DMFT≥8 (aOR, 1.41; 95% CI, 1.07 to 1.84; p=0.014). Heavy smoking was associated with a higher risk of DMFT≥8 in males (aOR, 1.38; 95% CI, 1.25 to 1.52; p<0.001) and females (aOR, 1.24; 95% CI, 1.03 to 1.50; p=0.022).
Conclusions
Tobacco smoking was associated with dental caries in the Indonesian population.
INTRODUCTION
Dental caries, the most prevalent non-communicable disease worldwide, affects individuals of all ages, from infants to the elderly. Its global prevalence has elevated it to a significant public health concern, given its preventability and widespread occurrence. Dental caries can lead to pain, difficulty eating and sleeping, and chronic systemic infection. It impacts not only a vast number of people across all age groups, but also individuals of all socioeconomic statuses, affecting their health, well-being, and social interactions [1]. According to the Global Burden of Disease Study 2019, dental and oral health issues, particularly dental caries, afflict nearly half of the global population, equating to approximately 3.58 billion people [2]. The Basic Health Research (Riskesdas) report of 2018 revealed that the prevalence of dental caries in Indonesia stands at 88.8% [3]. Dental caries arises from the production of acidogenic bacterial acids. These acids form and proliferate in plaque biofilms and fermentable sugars, leading to progressive tooth damage [4]. If left untreated, dental caries can cause significant pain and discomfort, ultimately resulting in tooth loss [2,5].
Dental health is intimately tied to quality of life, encompassing a range of factors such as demographic elements, psychological aspects, oral hygiene practices, oral health behaviors, and socioeconomic status [6]. Dental caries is a multifactorial disease influenced by physical and biological elements, lifestyle choices, oral health habits, and social standing [7]. The prevalence of dental caries is associated with lifestyle factors, including dietary habits such as sugar consumption [8]. Recent studies have shown that dental caries is associated with smoking [9,10] and tooth brushing [11]. Dental caries is also associated with a higher body mass index [12] and metabolic syndrome [13]. Given the high number of patients with dental caries, the cost of treatment represents a significant health burden. The global economic impact of dental caries is estimated to be around US dollar (USD) 442 billion annually, with USD 298 billion going towards treatment costs and USD 144 billion related to lost workdays [14].
While the risk of developing dental caries spans all age groups, most studies on this topic have focused primarily on children or toddlers. Numerous risk factors influence the prevalence of dental caries in children, including diet, oral hygiene, feeding practices, low birth weight, hereditary enamel defects, maternal education, family knowledge of dental and oral health, attitudes and practices, household income level, socio-cultural, environmental, and economic factors [15]. There have been several studies on dental caries in age groups other than children and toddlers [10,12–14], but research on individuals over the age of 10 remains limited. This study, therefore, explored the determinants of dental caries in the Indonesian population, ranging in age from 10 years to over 65 years. It not only described the incidence of dental caries in this age group, the respondents’ backgrounds, and proper tooth brushing techniques, but also examined consumption and smoking behaviors, with separate analyses based on sex. All factors contributing to caries were incorporated into a multivariate logistic regression analysis. This research represents an in-depth analysis of data from national studies conducted in Indonesia in 2018.
METHODS
Study Design and Participants
This study represents an extended analysis of the cross-sectional Community Indonesian Health Survey, also known as Basic Health Research (Riskesdas), conducted in 2018. The research measured indicators such as health status, which included dental conditions, and risk factors, which encompassed health behavior. The study population comprised all households across 34 provinces and 514 districts/cities in Indonesia, as derived from the 2018 National Socioeconomic Survey (National Statistics Bureau) sample frame database, which was conducted in March 2018. To select 30 000 census blocks and ten households, a method known as probability proportional to size was employed. This method involved systematic sampling with the highest implicit stratification of education completed by the head of household in each census block. Data were gathered from all individuals, regardless of age, in the selected households. As a result, data were collected from 1 091 528 individuals of all ages across 282 654 successfully interviewed households. A dental and oral examination was included as a subsample of the Riskesdas 2018, providing a national level of representation. This dental and oral examination was successfully conducted in 19 553 households across 2490 census blocks out of a targeted 25 000 census blocks in 26 provinces [3].
The inclusion criteria for this study were respondents aged 10 years and over who underwent dental examinations and had smoking behavior data, as well as information on other covariates. Out of the 37 026 participants who were 10 years or older, 4076 did not have dental examinations, and 2441 did not have complete smoking data, making it impossible to calculate their Brinkman index. Therefore, the final sample consisted of 35 391 individuals.
Data Collection
The subjects of this study were males and females aged 10 years and older, who were surveyed in the Indonesian Health Study. The gathered data encompassed demographic details, results of dental and oral examinations, and information on health-related behaviors. Trained health professionals conducted face-to-face interviews with the respondents in their homes. Dental and oral examinations were performed by dentists at specified health facilities.
A dentist conducted an intraoral examination utilizing a mouth mirror, probe, and sterile tweezers. Prior to the examination, respondents were instructed to rinse their mouths. Respondents were classified as having dental caries if cavities (D), missing teeth (M), or fillings (F) were detected in one or more teeth (T). Subsequently, the dentist recorded the DMFT score. The gathered data were documented in a paper questionnaire before being inputted into a computer. To guarantee data quality, a designated individual at the district/city level supervised the data collection process in the field.
The dependent variable of this study was the DMFT status at the time of the examination. Subjects were classified as having severe dental caries if they fell within the top 30% of the population in terms of DMFT values [16]. The cut-off point for severe dental caries in this study was determined according to the methods of the University of Malmo and Leake et al. [17]. Participants in the study were ranked according to their individual DMFT scores. Those comprising approximately the top third of the sample, with the highest DMFT scores, were identified as having severe dental caries. The lowest DMFT score among these participants was 8. Consequently, for the purposes of this study, severe dental caries was operationally defined as a DMFT score ≥8.
In this study, the primary independent variable was smoking activity, evaluated both qualitatively (smoking status: never smoked, ex-smoker, and active smoker) and quantitatively (amount of cigarette exposure). The Brinkman index (BI) was used to classify smoking exposure. The BI is a measure of smoking exposure, calculated by multiplying the average number of cigarettes smoked per day by the number of years the individual has been smoking. For the purposes of this study, heavy smokers were defined as those with a BI of 400 or more [18]. Based on their exposure to cigarettes, participants were categorized into three groups: (1) never smoked (BI, 0); (2) light smokers (BI, 1–399); and (3) heavy smokers (BI≥400).
In addition to the dependent and independent variables, we also included covariate variables. These variables consisted of demographic characteristics such as sex, age, level of education, occupation, geographic location, and socioeconomic quintiles. Other variables included proper toothbrushing behavior, and the consumption of sweet foods, sweetened drinks, soft drinks, and energy drinks. The respondents’ ages at the time of the study were categorized into the following groups: 10–14 years, 15–24 years, 25–34 years, 35–44 years, 45–54 years, 55–64 years, and 65 years and older. Education levels were classified based on the highest level of schooling completed by the participants (elementary school or less, middle school, high school, and college or above) [19]. Occupations were categorized as follows: army/police/government/private employees, merchants, laborers, unemployed, and others. Geographic location was divided into two categories: rural and urban. Socioeconomic quintiles were determined based on the index of household goods ownership, and were divided into 5 groups: quintile 1 (highest) to quintile 5 (lowest). Proper toothbrushing behavior was categorized as either “yes” or “no.” A “yes” response indicated that toothbrushing was done after breakfast and before bed, while a “no” response indicated the opposite. Food consumption patterns were determined based on frequency of consumption, as follows: up to 2 times per week, and from 3 times a week to more than once per day.
Statistical Analysis
A descriptive analysis was carried out to illustrate the sample distribution based on various characteristics. The chi-square test was utilized in the data analysis to investigate the correlation between severe dental caries and smoking exposure. Multivariate logistic regression models were employed to estimate the association between the dental caries severity (DMFT) with smoking exposure and smoking status at the 5% significance level. Multivariate logistic regression also allows the estimation of the adjusted odds ratio (aOR) between the desired outcome and the covariate factors. The covariates in the multivariate model were variables with p-values less than 0.05 in the bivariate stage for the overall, male, and female patterns, respectively. The covariates included in the overall model are age, education level, occupation, geographic location, proper toothbrushing habits, and consumption of sweet foods, soft drinks, and energy drinks. For the male model, the covariates were age, education level, occupation, geographic location, proper toothbrushing habits, and consumption of sweet foods, sweetened drinks, soft drinks, and energy drinks. In the female model, the covariates were age, education level, occupation, and consumption of sweet foods, soft drinks, and energy drinks. All analyses were conducted using SPSS version 15.0 (SPSS Inc., Chicago, IL, USA).
Ethics Statement
The Commission of Health Research granted ethical clearance for this study (National Institute of Health Research and Development, Indonesian Ministry of Health No. LB.02.01/2/KE.267/2017).
RESULTS
Table 1 shows that the majority of the research sample was drawn from the productive age group of 25–54 years old, accounting for 55.7% of the total. The sample was predominantly female (59.0%) and comprised elementary school graduates (51.7%). The sample was almost evenly split between the unemployed (49.2%) and laborers (23.7%). Nearly half of the sample was classified as wealthy (44.6%), and a significant majority resided in urban areas (64.9%). Furthermore, 23.4% of the sample were current smokers, while 4.1% were former smokers. Notably, 26.4% of the sample fell into the heavy smoking category, with a BI exceeding 400.

Socio-demographic characteristics of Indonesians aged 10 years and older – Basic Health Research, 2018
Table 2 demonstrates that 36.0% of the population had a DMFT score ≥8, with a slightly higher prevalence in females (37.5%) compared to males (33.9%). The proportion of individuals with a DMFT score ≥8 increased with age, for both males and females. Heavy smokers were more likely to have a DMFT score above 8 (41.8%), with 41.1% of these being male and 53.7% being female when considered separately. The distribution of DMFT scores ≥8 was fairly even across all education levels, but was most prevalent in the group that had never attended school or had no formal education. For males, a DMFT score ≥8 was primarily observed in laborers and other similar occupations. The same was true for females, where a DMFT score ≥8 was most common among workers, entrepreneurs, and other similar groups. Individuals residing in rural areas were more likely to have a DMFT score ≥8 than those living in urban areas.

DMFT conditions according to characteristics and sex– Basic Health Research 2018
The results of the multivariate logistic regression, as shown in Tables 3 and 4, indicate that active smokers generally had a 6.8% increased risk of having a DMFT score ≥8 (aOR, 1.07; 95% CI, 1.00 to 1.14; p=0.037). This trend was also observed in male smokers (aOR, 1.40; 95% CI, 1.27 to 1.55; p<0.001), and male ex-smokers (aOR, 1.18; 95% CI, 1.01 to 1.38; p=0.034). Females who had previously smoked (ex-smokers) had a 41% increased risk of having a DMFT score ≥8 (aOR, 1.41; 95% CI, 1.07 to 1.84; p=0.014). Among males, heavy smoking was associated with a 38% increased risk of having a DMFT score ≥8 (aOR, 1.38; 95% CI, 1.25 to 1.52; p<0.001), while in females, the risk was increased by 24% (aOR, 1.24; 95% CI, 1.03 to 1.50; p=0.022). The probability of having a DMFT score ≥8 increases with age, both overall and when broken down by sex. Occupations other than army, police, government, or private sector employees were associated with a higher risk of having a DMFT score ≥8, particularly in the overall sample and among males. Consumption of sweet foods was linked to a higher risk of having a DMFT score ≥8, both overall and when analyzed by sex. Similarly, the consumption of sweet drinks is associated with a higher risk, especially among males.

Multivariate logistic regression smoking status and DMFT status ≥8
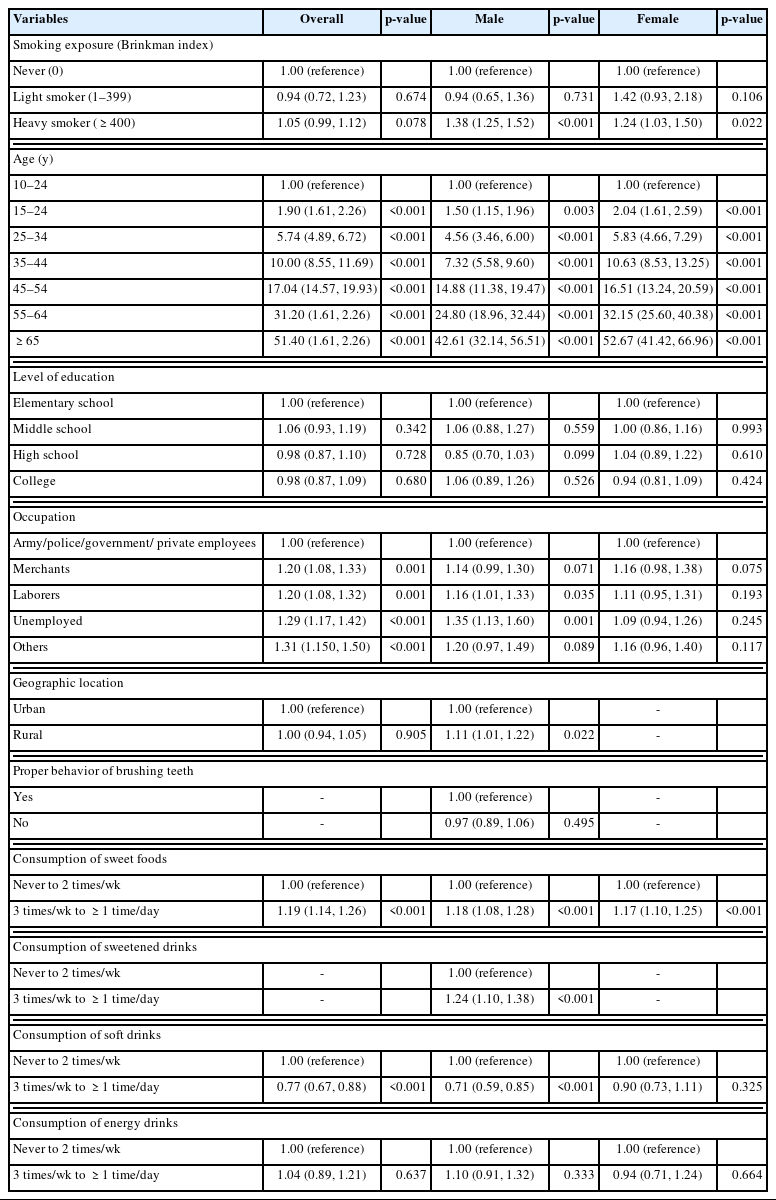
Multivariate logistic regression smoking exposure (Brinkman index) and DMFT status ≥8
Multivariate analysis, segmented by age group, revealed that smokers were more likely to experience DMFT scores ≥8 within the age group of 25–34 years, 35–44 years, and 55–64 years. However, both former smokers and heavy smokers were more likely to experience DMFT scores ≥8 within the age group of 35–44 years and 55–64 years. Light smokers, however, were more likely to experience these scores within the 35–44 years age group (Table 4).
DISCUSSION
Smoking habits in Indonesia are on the rise, with a significant increase observed year after year (Riskesdas, 2018). The 2012 Indonesia Demographic and Health Survey analysis revealed that males smoked more than females [20]. Consequently, the analysis was conducted separately for each sex to yield more accurate results. The findings indicated that severe dental caries (DMFT≥8) were associated with factors such as age, occupation, consumption of sweet foods, soft drinks, and smoking habits in both males and females. However, geographic location and the consumption of sweetened drinks were only associated with males.
This study revealed a correlation between DMFT and age, with older age groups experiencing a higher incidence of dental caries. Research on DMFT in children has demonstrated a relatively high percentage that increases with age. A study conducted in Saudi Arabia also indicated that dental caries is a significant public health issue among children [6]. This is partially attributed to increasingly complex consumption patterns as children age. Numerous studies have established a link between an individual’s diet, particularly the consumption of sugary foods and beverages, and dental caries. The primary risk factor for dental caries is the consumption of sugary foods and drinks, which can double the risk of developing this condition [15]. The lack of availability of high-quality food and the proliferation of sugary and fatty foods that are low in energy and nutrients are among the factors driving changes in consumption behavior patterns [21]. This study also found that, in addition to sugary foods, soft drinks contribute to dental caries. Male respondents who frequently consumed energy drinks were more likely to develop dental caries than those who did not. This could be attributed to the high carbohydrate content in sugar, which can linger on the teeth and provide a breeding ground for bacteria [1,14].
The dietary choices people make are shaped by a multitude of intricate factors, including socioeconomic status, education, and occupation. Our research indicates that education and occupation significantly impact DMFT scores. Both males and females who have never received formal education exhibit the highest percentage of DMFT. Furthermore, labor-intensive occupations correspond with the highest percentage of DMFT. These findings align with previous studies that have identified a correlation between education and dental health, with those only having primary education experiencing a 25% increased risk, and illiteracy correlating with the highest risk. This significant correlation is closely tied to the formation of attitudes and perceptions, as well as the influence of the family environment on dental and oral health [15].
Numerous epidemiological studies worldwide have established a strong correlation between smoking and the incidence of periodontitis and dental caries [9,10,22]. Smoking heightens the risk of gum disease and oral cancer. It can also lead to tooth discoloration (staining), bad breath, and interference with the wound-healing process in periodontal disease. A study conducted in Scotland demonstrated that children born to mothers who smoked during pregnancy have a higher prevalence of caries compared to those born to non-smoking mothers [13]. In Portugal, smoking has been identified as a risk factor for dental caries, with a 7% reduction in caries incidence observed when exposure to cigarettes is avoided [23]. A systematic review by Benedetti et al. [24] further corroborates that tobacco smoking is closely associated with an increased risk of caries.
In Indonesia, dental caries are more prevalent among heavy smokers compared to those who have never smoked [25]. This observation is consistent with the findings of Sumartono et al. [25], which also indicated a higher incidence of dental caries among individuals with greater exposure to cigarettes. For smokers, the mouth and teeth are the initial points of contact with tobacco. The constituents of cigarettes subsequently promote the proliferation of carcinogenic microorganisms. These bacteria, known to instigate caries, generate acid in the oral cavity by breaking down fermentable carbohydrates through enzyme secretion or metabolism, leading to further demineralization of dental hard tissues. Given that about 7000 distinct molecules are inhaled from cigarettes, it is challenging to pinpoint which component has the most substantial impact on caries-associated bacteria [9].
Previous research has demonstrated that smoking can diminish the buffering capacity of saliva, leading to a decrease in salivary pH [26]. In addition, smoking also affects the concentration of salivary proteins such as salivary secretory IgA (sIgA) and amylase [27,28]. sIgA plays a crucial role in defending against oral and dental diseases by inhibiting the adherence of microbes to tooth surfaces and oral epithelial cells. A reduced sIgA concentration is a risk factor for dental caries in both children and adults. The immunosuppressive properties of smoking, which are dose-dependent, are evident in the reduced concentration of sIgA in the saliva of adult smokers and children exposed to secondhand smoke.
Amylase plays a vital role in streptococcal colonization and metabolism, which contributes to the development of dental caries. It functions as a receptor on the pellicle, providing a surface for bacteria to attach to the tooth. Prior research has indicated that individuals who smoke tend to have higher concentrations of salivary amylase. This enzyme can elevate the pH level of dental plaque, thereby encouraging the colonization of oral microbiota and heightening the risk of caries [29].
There are limitations to this study. We carried out a population-based cross-sectional study, the results of which cannot establish a cause-and-effect relationship between dental caries and tobacco smoking in the Indonesian population. As such, we recognize the need for a more robust study design to ascertain whether heavy smoking could potentially lead to severe dental caries. A prospective cohort study could be one such option.
Notes
CONFLICT OF INTEREST
The authors have no conflicts of interest associated with the material presented in this paper.
FUNDING
None.
AUTHOR CONTRIBUTIONS
Conceptualization: Andayasari L, Mubasyiroh R, Sufiawati I, Data curation: Mubasyiroh R, Andayasari L. Formal analysis: Mubasyiroh R, Andayasari L, Sufiawati I. Funding acquisition: None. Methodology: Mubasyiroh R, Andayasari L, Nurlinawati I. Visualization: Sufiawati I. Writing – original draft: Andayasari L, Mubasyiroh R. Writing – review & editing: Andayasari L, Nurlinawati I, Mubasyiroh R, Sufiawati I.
ACKNOWLEDGEMENTS
The authors thank the Head of the National Institute of Health Research and Development, Ministry of Health, the Republic of Indonesia, for permission to use Basic Health Research 2018 data in this study.