Environmental Health Literacy Regarding Fine Particulate Matter and Related Factors Among Village Health Volunteers in Upper Northern Thailand
Article information

Abstract
Objectives:
Fine particulate matter pollution has emerged as a significant life-threatening issue in Thailand. Recognizing the importance of environmental health literacy (EHL) in disease prevention is crucial for protecting public health. This study investigated EHL levels and aimed to identify associated factors among village health volunteers (VHVs) in the upper northern region of Thailand.
Methods:
A cross-sectional study was conducted to collect data from 710 VHVs using the EHL assessment tool developed by the Department of Health, Thailand.
Results:
The overall EHL score was moderate (mean, 3.28 out of a possible 5.0), with the highest and lowest domain-specific mean score for the ability to make decisions (3.52) and the ability to access (3.03). Multiple linear regression revealed that the factors associated with EHL score were area of residence (urban areas in Chiang Mai: B=0.254; urban areas in Lampang: B=0.274; and rural areas in Lampang: B=0.250 compared to rural areas in Chiang Mai), higher education levels (senior high school: B=0.212; diploma/high vocational certificate: B=0.350; bachelor’s degree or above: B=0.528 compared to elementary school or lower), having annual health checkups compared to not having annual health check-ups (B=0.142), monthly family income (B=0.004), and individuals frequently facing air pollution issues around their residence (B=0.199) compared to those who reported no such issues.
Conclusions:
The VHVs exhibited moderate EHL associated with residence area, education, health check-ups, family income, and residential air pollution. Considering these factors is vital for enhancing VHVs’ EHL through strategic interventions.
INTRODUCTION
Air pollution is the leading environmental factor contributing to global disease burden and premature mortality. Each year, over 13 million deaths are attributed to preventable environmental causes [1]. The combined effects of ambient and household air pollution result in approximately 7 million premature deaths annually, with countless individuals experiencing health problems from inhaling polluted air [1,2]. Developing countries are disproportionately affected, with these nations accounting for more than half of the total death toll [1,3-5]. Among these risks, particulate matter with a diameter of less than 2.5 µm (PM2.5) is a major concern globally [6]. Numerous scientific studies have linked exposure to particle pollution to various health issues, including premature death, heart or lung diseases, non-fatal heart attacks, irregular heartbeat, aggravated asthma, decreased lung function, and respiratory symptoms such as irritation of the airways, coughing, or difficulty breathing [1,2,6,7].
According to the 2021 World Air Quality Report, East Asia, Southeast Asia, and South Asia had the highest annual average PM2.5 concentrations when adjusted for population [8]. Open burning is estimated to account for a significant 5% to 30% of the total man-made emissions in Southeast Asia [9]. Thailand was ranked fifth among countries in the region and 45th globally [8]. The upper northern region of Thailand is plagued by a seasonal haze crisis that recurs during the winter and early summer months [10]. This persistent haze, particularly in basin-like terrains under dry and stable atmospheric conditions, leads to detrimental effects on environmental quality and public health. An analysis of PM2.5 measurements in 2021 revealed that the upper northern region frequently exceeded the established air quality standards [11].
Environmental health literacy (EHL) refers to the ability to forge significant links between environmental exposures and human health outcomes [12]. This intellectual skill encompasses the active pursuit, comprehension, evaluation, and application of environmental health information to make informed decisions, minimize health risks, improve quality of life, and protect the environment [13-15]. Mastery of EHL can lead to a thorough understanding of specific risks and is recognized as a dynamic process. Through this process, individuals and communities gradually gain knowledge about environmental and health risks, exposures, outcomes, and strategies to counteract negative environmental impacts while simultaneously promoting health [16-18]. Efforts to mitigate the health effects of air pollution requires coordinated efforts from public authorities at national, regional, and international levels [18]. In Thailand, village health volunteers (VHVs) play a major role in disseminating vital public health information and messages to community members, especially during outbreaks or epidemics. VHVs are skilled communicators in the local language and demonstrate a profound respect for local cultural and religious practices [19,20]. They play a key role in educating the community about the health risks associated with air pollution and in providing advice on protective measures to reduce exposure, particularly for at-risk groups. These measures include recommending staying indoors and limiting physical activity when air quality is poor [21].
Previous studies in various countries have thoroughly investigated PM2.5 health literacy assessments at both the national level and within specific populations, employing research tools designed to meet their respective objectives [17,22-25]. Several factors have been identified as key determinants influencing different aspects of EHL; however, not all factors have shown significant correlations [13,17,22-24,26,27]. EHL has the potential to enable VHVs to lead community environmental management efforts, enhancing awareness and promoting effective collaboration [13,19]. Despite this, research evaluating EHL among VHVs is scarce, particularly in areas with high PM2.5 concentrations, such as the upper northern region of Thailand. Therefore, the main aim of this study was to evaluate EHL levels pertaining to fine particulate matter and its influencing factors among VHVs in this region. The findings of this study will offer valuable insights for policymakers, aiding in the development of targeted interventions to minimize EHL disparities across different demographic groups.
METHODS
Study Design and Setting
This study employed a cross-sectional design, focusing on VHVs in the upper northern region of Thailand during July 2023 and August 2023. The study used a combination of purposive and convenience sampling techniques in the following sequence: Initially, the provinces of Chiang Mai and Lampang were purposively selected based on their high number of days with PM2.5 levels exceeding the Thailand ambient air quality standards in 2021, according to which the 24-hour average of PM2.5 must not exceed 50 µg/m3 [11]. Subsequently, the area cluster method was utilized to divide the administrative districts in each province, selecting one rural and one urban district from each. Within these districts, four sub-districts were chosen. For the recruitment of participants, convenience sampling was employed, yielding approximately 45-46 VHVs per sub-district.
Participants and Sample Size
The sample size estimation for the initial phase of developing a health literacy enhancement program aimed at fine particulate matter prevention for VHVs in upper northern Thailand was conducted using a cross-sectional study design. Cochran’s proportion formula [28] was utilized to calculate the necessary sample size. Several key parameters informed this calculation: a proportion of 0.686 [26], a 95% confidence level, and a 5% margin of error [29]. To accommodate the complexities of the sampling design, a design effect of 2 was incorporated, yielding a sample size of 661 participants. Given that data collection was based on self-administered questionnaires and relied on voluntary participation, the potential for incomplete responses was recognized. To account for this, a non-response rate of 10% was included in the sample size calculation, increasing the total number of participants to 728 for the study. The inclusion criteria required that participants be active VHVs who had lived in the study area for at least 1 year. They also needed to express a willingness to participate in the research and have adequate reading, writing, and listening skills in Thai. Any individuals with incomplete data were excluded from the analysis.
Instruments
The questionnaire utilized in this study was divided into two sections. The first section collected general demographic information about the participants, covering variables such as geographic area of residence, gender, age, body mass index (BMI), education level, occupation, underlying diseases, allergies, frequency of annual health check-ups, years of experience as VHVs, primary language, household size, monthly family income, perceived adequacy of family income, and local air pollution issues. The inclusion of these particular factors was informed by prior academic research [13,17,22-24,26,27], which ensured their relevance to the context of this study and contributed to its overall validity and applicability.
The second section of the questionnaire was derived from the EHL assessment on PM2.5, which was developed by the Health Impact Assessment Division of the Department of Health in Thailand [13]. This section was based on the conceptual framework of EHL as proposed by Gray [15] and Marsili et al. [14]. It consists of 28 items, evenly divided into four domains with seven items each. These domains assess the ability to access, understand, evaluate, and make decisions using environmental health information to protect against PM2.5 exposure. Participants provided their responses on a 5-point Likert scale, with options ranging from strongly disagree (1 point) to strongly agree (5 points). The scores were then converted into percentages, with specific thresholds used to categorize EHL levels: scores below 60% (mean, 1.00-3.00) were considered indicative of low EHL, scores between 60% and 80% (mean, 3.01-4.00) suggested moderate EHL, and scores above 80% (mean, 4.01-5.00) were classified as high EHL. This assessment tool had been previously used with VHVs in an eco-industrial town in central Thailand. The questionnaire was also developed in collaboration with three experts in behavioral health research and measurement to ensure its validity and comprehensiveness. The index for item objective congruence was above 0.5, the reliability coefficient ranged from 0.80 to 0.95, the power of discrimination was between 0.26 and 0.84, and the factor loading varied from 0.50 to 0.84 [13].
Statistical Analysis
The data collected in this study were meticulously organized and analyzed using SPSS version 29.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were used to investigate the study variables. We employed a simple linear regression model to identify potential factors associated with EHL. Variables with a p-value of less than 0.15 were considered for inclusion in the multiple linear regression analysis. Only variables with statistical significance at the alpha level of 0.05 were presented in the final model. A variance inflation factor value of less than 5 indicated the absence of multicollinearity [30].
Ethics Statement
This study strictly adhered to the ethical principles outlined in the Declaration of Helsinki. Approval and ethical clearance were obtained from the Faculty of Public Health Research Ethics Committee on Human Research at Chiang Mai University, with the assigned institutional review board approval number Ref. No. ET018/2023. Written consent was obtained from all participants in the study after they received a thorough explanation of the study’s nature and objectives.
RESULTS
In this study, a total of 710 VHVs participated. Of these, 361 individuals (50.8%) were recruited from Chiang Mai province, with an equal distribution between urban (25.6%) and rural (25.2%) districts. The remaining 349 individuals (49.2%) came from Lampang province, where 20.9% were from urban districts and 28.3% from rural districts. The majority of participants were women, making up 80.4% of the total, while men represented 19.6%. Nearly half of the participants (47.2%) reported having underlying diseases, and a small percentage (4.2%) reported allergies. On average, participants had 14.8±10.2 years of experience as VHVs. Most participants (62.7%) spoke Northern Thai as their primary language, and the median number of family members was four. In terms of air pollution issues around their homes, 35.0% of the participants reported occasional problems, while 40.6% reported frequent problems (Table 1).

Demographic characteristics of village health volunteers
The participants’ overall EHL was found to be at a moderate level, with mean scores ranging from 3.03 to 3.52 out of a possible 5.0. Within the various domains assessed, the ability to access environmental health information had the lowest mean score of 3.03±0.97. In contrast, the ability to make decisions based on the information received the highest mean score of 3.52±0.85. The study indicated that just over half of the participants (52.5%) rated their EHL as moderate, while a small minority (13.9%) viewed themselves as highly proficient. Concerningly, more than half of the participants (51.8%) reported low EHL when it came to accessing environmental health information, as shown in Table 2.
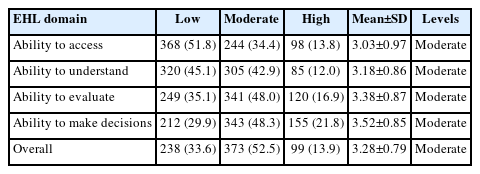
Distribution of EHL regarding PM2.5
Linear regression analyses were conducted to investigate the variables associated with EHL on PM2.5. In the univariable analysis, several factors were examined, including geographic area of residence, education level, occupation, underlying diseases, annual health check-ups, primary language, family income, sufficiency of family income, and the presence of air pollution problems around the residence. These factors showed significant associations with EHL, each with a p-value of less than 0.15. Subsequently, all nine variables were included in the multivariable analysis (Table 3).

Relationship between predictors and EHL regarding PM2.5 among VHVs using simple linear regression
The final results of the multiple linear regression analysis indicated that several factors were significantly associated with EHL, with a p-value less than 0.05. These factors included geographic area of residence, level of education, frequency of annual health check-ups, monthly family income, and the presence of air pollution problems around the residence. Specifically, VHVs living in the urban district of Chiang Mai (B=0.254; p<0.01), the rural district of Lampang (B=0.250; p<0.01), and the urban district of Lampang (B=0.274; p=0.001) had significantly higher EHL scores compared to those in the rural district of Chiang Mai. Additionally, VHVs with higher educational attainments, such as senior high school (B=0.212; p<0.01), diploma/high vocational certificate (B=0.350; p<0.01), and bachelor’s degrees or higher (B=0.528; p<0.001), were found to have higher EHL scores. VHVs who participated in annual health check-ups also had higher EHL scores (B=0.142; p<0.05). A positive correlation was observed between monthly family income and EHL (B=0.004; p<0.05). Notably, VHVs living in areas with frequent air pollution problems reported higher EHL scores than those without such issues (B=0.199; p<0.01) (Table 4).

Relationship between predictors and EHL regarding PM2.5 among VHVs using multiple linear regression
When categorized by geographic area of residence, the multiple linear regression analysis revealed that education levels significantly influence EHL, with higher education correlating with greater literacy in both districts, especially in the urban areas of Chiang Mai and Lampang. In Lampang’s rural district, having annual health check-ups is positively associated with EHL, whereas monthly family income is a significant factor in the rural areas of Chiang Mai. Furthermore, the presence of air pollution problems in the vicinity of one’s residence is consistently linked with higher EHL in the rural district of Lampang, highlighting the importance of local environmental factors (Table 5).

Coefficients in multiple regression analyzing the relationship between factors and EHL regarding PM2.5 among VHVs classified by geographic areas
DISCUSSION
The present study aimed to evaluate the levels of EHL and associated factors among VHVs in the upper northern region of Thailand. Our findings indicate that the overall EHL level among participants was moderate. However, it is concerning that approximately one-third of the participants displayed low EHL. Additionally, the results show that all domains of EHL were at a moderate level, with mean scores ranging from 3.03 to 3.52 on a 5-point scale. Of these domains, the ability to access information had the lowest mean score, while the ability to make decisions had the highest. Our findings are consistent with previous studies conducted in an eco-industrial town in central Thailand (Ratchaburi, Samut Sakhon, Nakhon Pathom, Rayong, Chonburi), which also found that the majority of participants had moderate EHL [13,26]. Similarly, our results align with a study from Bueng Kan, Northeast Thailand, where the mean EHL score of participants was determined to be moderate [27]. These commonalities across different regions of Thailand highlight the importance of addressing EHL to promote sustainable practices and improve public health outcomes. When comparing our results with those from other countries using different EHL measurement tools, our study’s outcomes are in line with research among adult residents of Taiwan, where similar EHL levels were reported [22]. However, there is a notable difference with a study from China, which found the overall EHL level to be low [23]. This indicates that EHL levels can vary significantly between different countries or regions, potentially due to a variety of factors such as educational levels, the presence or absence of awareness campaigns, and cultural differences. Furthermore, variations in the tools or instruments used to measure EHL could influence the results, as there may be differences in design, content, and measurement methodologies across studies.
The research findings highlight significant disparities in EHL across districts. Individuals in the urban district of Chiang Mai, as well as both the rural and urban districts of Lampang, showed higher levels of EHL compared to their counterparts in Chiang Mai’s rural district, which is home to a minority group. This observation is consistent with a study conducted in China, which found that rural residents had significantly lower EHL than those living in urban areas [23,31]. These results suggest that geographical location may play a role in influencing EHL levels among participants. Furthermore, multiple linear regression analysis, when categorized by geographic area of residence, reveals that a variety of factors are significantly associated with EHL in different regions. These findings highlight the array of factors that affect EHL and underscore the importance of designing interventions that are tailored to the specific needs of different areas.
The study found a positive association between higher education levels and enhanced EHL. This aligns with existing research that demonstrates a strong link between education and health literacy [23,31,32]. However, it is important to recognize that individuals with lower educational levels can also possess EHL. Tailored outreach and educational programs that reach across different educational backgrounds can promote EHL, thereby making this critical knowledge accessible to a wider range of VHVs. Education plays a key role in equipping individuals to understand and address environmental health challenges, leading to more informed decision-making and improved public health outcomes [12,33-35]. It is particularly noteworthy that VHVs who participate in annual health checkups show higher levels of EHL. This compelling finding suggests a possible link between personal health awareness and environmental consciousness. The correlation may imply that individuals who take their health seriously are also more likely to seek out information on environmental factors that could affect their well-being [36,37].
A significant association was found between higher monthly family income and positive EHL outcomes in this study, indicating that a higher monthly family income correlates with a greater literacy score in this domain. This finding is consistent with a study from the United States, which also reported a positive relationship between income levels and EHL [35]. Similarly, research from Denmark showed that individuals with an annual income below the national average were more likely to have inadequate and limited health literacy [38]. These results suggest that higher income levels typically lead to better access to healthcare, healthier living conditions, and more resources to maintain a healthy lifestyle. Furthermore, the study identified a notable link between the presence of air pollution issues in one’s locality and increased levels of EHL. The data indicate that individuals who frequently encounter air pollution problems (described as “often”) have a significant and positive association with EHL, unlike those who never face air pollution issues. However, this positive association is not statistically significant for individuals who only sometimes experience air pollution issues (described as “sometimes”). It is important to note that this study is observational in nature, and while a statistical correlation is present, causation cannot be inferred. There may be other factors not considered in this study that could affect the relationship between air pollution issues and EHL. Further research and thorough analysis are essential to identify these potential factors.
The study has certain limitations that should be taken into account. First, the cross-sectional design limits our ability to establish causal relationships between the identified factors and EHL. Longitudinal studies or experimental designs would be more appropriate for determining causality. Second, the use of self-reported questionnaires may introduce social desirability bias, with participants potentially providing responses they believe to be more favorable. Although steps were taken to ensure anonymity and confidentiality, it is not possible to completely eliminate inherent biases. Third, the study is limited to VHVs in the upper northern region of Thailand, which may limit the generalizability of the findings to other populations or regions. Conducting the study in various settings could enhance the external validity of the results. Finally, relying on a single EHL assessment tool may not capture all aspects of EHL. Future research should consider using both qualitative and quantitative methods to gain a more holistic understanding of EHL among VHVs and to investigate additional dimensions not covered by the current tool.
In conclusion, this study revealed that VHVs in the upper northern region of Thailand exhibited a moderate level of EHL. Significant associations with EHL were observed in relation to geographic areas of residence, education level, frequency of annual health check-ups, monthly family income, and levels of air pollution around their residences. Therefore, policymakers and healthcare providers should consider these factors when developing strategies and interventions to enhance EHL among VHVs.
Notes
Conflict of Interest
The authors have no conflicts of interest associated with the material presented in this paper.
Funding
None.
Author Contributions
Conceptualization: Pansakun N, Naksen W, Boonchieng W, Ong-Artborirak P, Prapamontol T. Data curation: Pansakun N, Naksen W, Prapamontol T. Formal analysis: Pansakun N, Naksen W, Ong-Artborirak P. Funding acquisition: None. Methodology: Pansakun N, Naksen W, Boonchieng W, Ong-Artborirak P. Project administration: Pansakun N, Naksen W. Visualization: Pansakun N, Naksen W, Boonchieng W, Ong-Artborirak P. Writing – original draft: Pansakun N. Writing – review & editing: Pansakun N, Naksen W, Boonchieng W, Ong-Artborirak P, Prapamontol T.
Acknowledgements
The researchers express their sincere gratitude to the Graduate School of Chiang Mai University for their generous provision of Teaching Assistant and Research Assistant Scholarships, which have greatly supported the researchers in their endeavors. Furthermore, the researchers wish to acknowledgment the Faculty of Public Health at Chiang Mai University for their valuable support throughout this study, including their assistance in facilitating the issuance of an official letter.