Prevalence of Positive Carriage of Tuberculosis, Methicillin-resistant Staphylococcus aureus, and Vancomycin-resistant Enterococci in Patients Transported by Ambulance: A Single Center Observational Study
Article information
Abstract
Objectives
An ambulance can be a potential source of contagious or droplet infection of a community. We estimated the prevalence of positive carriage of tuberculosis (TB), methicillin-resistant Staphylococcus aureus (MRSA), and vancomycin-resistant Enterococci (VRE) in patients transported by ambulance.
Methods
This was a retrospective observational study. We enrolled all patients who visited a tertiary teaching hospital emergency department (ED). Blood, sputum, urine, body fluid, and rectal swab samples were taken from patients when they were suspected of TB, MRSA, or VRE in the ED. The patients were categorized into three groups: pre-hospital ambulance (PA) group; inter-facility ambulance (IA) group; and non-ambulance (NA) group. Adjusted odds ratio (OR) and 95% confidence intervals (CI) were calculated using a multivariable logistic regression model for the prevalence of each infection.
Results
The total number of patients was 89206. Of these, 9378 (10.5%) and 4799 (5.4%) were in the PA and IA group, respectively. The prevalence of TB, MRSA, and VRE infection were 0.3%, 1.1%, and 0.3%, respectively. In the PA group, the prevalence of TB, MRSA, and VRE were 0.3%, 1.8%, and 0.4%. In the IA group, the prevalence of TB, MRSA, and VRE were 0.7%, 4.6%, and 1.5%, respectively. The adjusted ORs (95% CI) of the PA and IA compared to the NA group were 1.02 (0.69 to 1.53) and 1.83 (1.24 to 2.71) for TB, 2.24 (1.87 to 2.69) and 5.47 (4.63 to 6.46) for MRSA, 2.59 (1.78 to 3.77) and 8.90 (6.52 to 12.14) for VRE, respectively.
Conclusions
A high prevalence of positive carriage of TB, MRSA, and VRE in patients transported by metropolitan ambulances was found.
INTRODUCTION
Community-acquired methicillin-resistant Staphylococcus aureus (MRSA) infection has increased as along with hospital-acquired MRSA all over the world. According to the US Centers for Disease Control and Prevention (CDC), the number of MRSA-associated admissions was 126 000 from 1999 to 2000 and the number cases of invasive MRSA was 94 360 cases in 2005, which brought with it very high associated medical costs [1,2]. In Canada, 8.62 per 1000 admissions in 2007 were MRSA-associated, and vancomycin-resistant Enterococci (VRE) was isolated in 1.32 patients per 1000 admissions [3]. MRSA and VRE are typical nosocomial infections and can be transmitted to healthy individuals via person to person contact. Thus, MRSA and VRE were designated as nationally notifiable communicable diseases by the Korea CDC since 2010 because of their infectivity and fatality. Tuberculosis (TB) has been a serious public health problem inducing endemic infection in Korea. In 2007, the incidence rate and mortality rate of TB in Korea were 71.6 and 5.9 per 100 000 persons respectively [4]. The World Health Organization estimated that 9.2 million new cases and 1.7 million deaths from TB occurred in 2006, of which 0.7 million cases and 0.2 million deaths were in Human immunodeficiency virus-positive people globally [5,6].
Numerous studies have reported that MRSA and VRE are common pathogens that can spread from patient to patient through surface contamination and healthcare workers [7]. TB can also be easily transmitted via the respiratory tract causing opportunistic infection, particularly in immune compromised patients.
Ambulances can be a potential source of contamination of various microorganisms because ambulances transport patients without having a prior knowledge of a patient's risk factors, or of the colonization or infection state of the ambulance. The space of an ambulance is small and closed, so there may be high probabilities of contamination between persons and between patients and equipment. A high call volume and lack of sufficient time for sterilization also make strict infection control difficult [8]. For these reasons, patients who are transported by ambulance are very vulnerable to infection. A high prevalence of infection among patients who are transported by ambulances is a risk factor of ongoing community transmission because it can be a source of infection of the next patient who is transported by the ambulance. We aimed to estimate the prevalence of positive carriage of TB, MRSA, and VRE among patients that present to the emergency department (ED) by mode of transportation.
METHODS
I. Study Design and Setting
This study was a retrospective observational study which was a review of patients' medical records among those who presented to the ED of one tertiary academic hospital. This study was reviewed and approved by the institutional review board of the study coordinating hospital and granted a waiver of signed informed consent.
This study was conducted at one tertiary academic hospital with 50000 annual visits and a 25% admission rate of ED visits. Pre-hospital ambulance services are operated by the fire department, which covers all emergency delivery. Inter-facility transports usually are performed by private ambulance companies. Ambulance crews in one delivery are composed of two or three, who have the license of emergency medical technician (EMT)-basic or EMT-intermediate. The ambulance authorities have their own infection control guidelines, which are declaratory rather than practical.
II. Data Collection and Processing
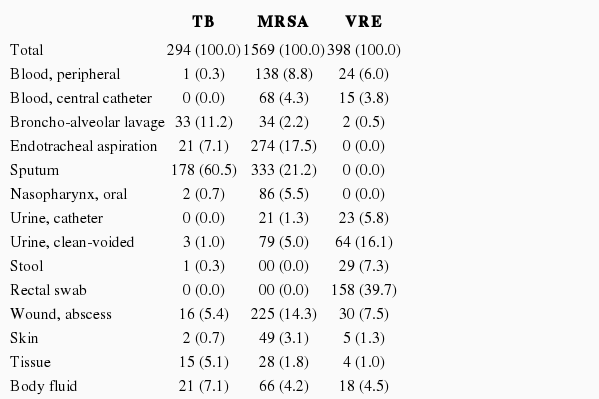
The patients who visited a study ED from January 2007 to December 2008 were enrolled. Doctors working in the ED ordered culture studies routinely when the patients had any sign of infection, such as fever, hypothermia, hypotension, leukocytosis, or elevation of c-reactive protein, although there are no standard rules for ordering cultures. Blood, sputum, urine, body fluid, and rectal swab samples were taken from patients when they were suspected of any infection in the ED.
Demographic data were extracted from the National Emergency Department Information System (NEDIS), which is a nationwide common registry for emergency patients. We collected the mode of transport to the ED from the NEDIS data, and we classified the study population according to their mode of transportation as the pre-hospital ambulance group, the inter-facility ambulance group, and the non-ambulance group. The microbiologic laboratory data was extracted from the microbiology registry of the study institute, which covered all microorganisms identified in ED patients as well as admitted patients. The data were selected using the time the sample was dropped off: the samples that were taken from patients immediately after arrival in the ED and before admission were included.
III. Outcome Measures and Data Analysis
For three microorganisms, the prevalence was calculated for all patients and for the ambulance utilization group. We determined the demographics of the groups, and we modeled the multivariable logistic regression analysis for the prevalence by the mode of visit (pre-hospital ambulance and inter-facility ambulance group) versus non-ambulance group adjusting for potential confounders. The adjusted odds ratio (OR) and 95% confidence intervals (CI) were calculated.
RESULTS
I. Demographic Findings
The total number of enrolled patients was 89 206. Of these, pre-hospital ambulances and inter-facility ambulances were used in 10.5% and 5.4% of patients, respectively. The median age of patients was 58 in the pre-hospital ambulance group, 62 in the inter-facility ambulance group, and 39 in the non-ambulance group. ED mortality was the highest in the inter-facility ambulance group (7.2%), followed by the pre-hospital ambulance group (1.9%) and the non-ambulance group (0.2%) (Table 1).
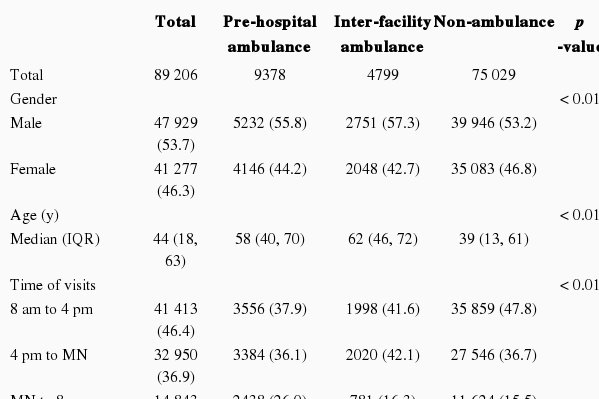
The characteristics of patients visiting the emergency department by type of transportation
II. Prevalence of Positive Carriage of TB, MRSA, and VRE
The prevalence of TB, MRSA, and VRE for all patients taken together were 0.3%, 1.1%, and 0.3%, respectively. TB was positive in 0.3% in the pre-hospital ambulance group and 0.7% in the inter-facility ambulance group and MRSA was positive in 1.8% in the pre-hospital ambulance group and 4.6% in the inter-facility ambulance group. VRE was positive in 0.4% in the pre-hospital ambulance group and 1.5% in the inter-facility ambulance group. There were statistical differences of age, gender, insurance, time and season of visit, and reason for visit between the positive and negative carriage of TB, MRSA, and VRE with older age, more ambulance use, and a higher proportion of disease as reason of visit in the positive cases (Table 2).
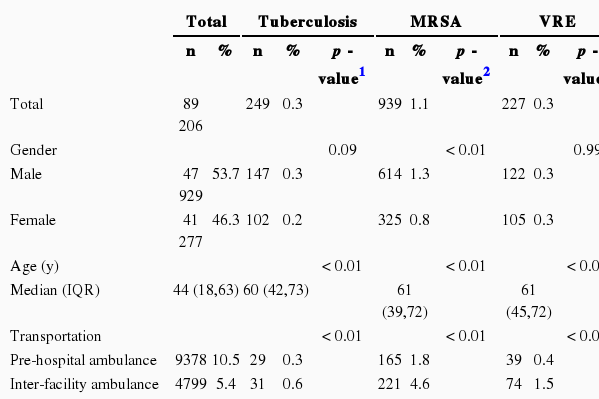
The characteristics of patients visiting the emergency department by type of infection
The adjusted ORs (95% CI) for the potential confounders of the pre-hospital ambulance group and inter-facility ambulance compared to the non-ambulance group were 1.02 (0.69 to 1.53) and 1.83 (1.24 to 2.71) for TB, 2.24 (1.87 to 2.69) and 5.47 (4.63 to 6.46) for MRSA, and 2.59 (1.78 to 3.77) and 8.90 (6.52 to 12.14) for VRE, respectively (Table 3).

Results of multivariable logistic regression model of tuberculosis, MRSA, and VRE infection by type of transportation
DISCUSSION
Antibiotic-resistant strains are an increasingly common and challenging public health issue in most of the world. In particular, MRSA is the most common strain of antibiotics-resistant infection, which varies in incidence according to geographic area and study institution. For example, Sweden and Norway reported less than 1% of MRSA, compared to high proportions in USA (25% to 50%), Canada (5% to 10%), and Hong Kong and Singapore (> 50%) [9]. VRE was reported at 7% in Germany and 16% in Switzerland and Greece [10]. In this study population, the overall prevalence of MRSA and VRE were 0.3% and 1.1%, which is not high compared to other countries. Although the incidence rates of TB have declined substantially in the United States, global efforts for TB control are being challenged by the steady increase in drug resistant TB, particularly multidrug resistant TB [11,12]. MRSA and VRE are also regarded as new challenging issues. Previous studies have reported that 51% to 59% of MRSA infections were found in purulent skin and soft tissue infections [13,14]. MRSA was found to be a potential risk factor with a 1.9 OR for the contamination of healthcare workers [13].
Several studies have reported positive MRSA findings in samples from ambulances [15-19]. These results also suggested that the patients with positive microorganisms who were transported by an ambulance could be a source of contamination of the ambulance. The ambulances which came into direct contact with patients were an important reservoir for these organisms. Furthermore, ambulances which transported the patients may be a potential risk factor of ongoing community transmission because it can be a source of infection to the next patients or ambulance crews who is transported by the ambulance. Regardless of whether the infection was community acquired or hospital acquired, therefore, patients with positive microorganisms who were transported by an ambulance can be another source of contamination of the ambulance, healthcare workers, and community contagion.
In particular, the inter-facility ambulance patients showed a much higher prevalence of MRSA and VRE than that in the ambulatory patients. The adjusted OR for MRSA of the pre-hospital ambulance group (2.24) was comparable with other studies, whereas the adjusted OR for MRSA of the inter-facility ambulance group (5.47) was very high. Patients who were transported from another hospital had a higher exposure to an infection risk of MRSA and VRE. It might be because there was no infection control program in the private ambulance services. Moreover, the patients transported between hospitals are more likely to be elderly and have a chronic disease or be in critical condition, and thus they are vulnerable for such infection. To decrease the spread of MRSA, patients with MRSA transported from another hospital were recommended to be isolated until being sterilized [20].
A higher rate of prevalence of MRSA and VRE does not always suggest that the ambulance is the source of contamination of community infection. However, these findings suggest that ambulance transport can be a potential source for infection for the next patients. To prevent this contagion, we should develop a strict infection control program for ambulance crews and services.
For ambulance infection control, the US Standard on Fire Department Occupational Safety and Health Program was introduced in 1987 [21,22]. To give enough ventilation in an ambulance, a strict ventilation time of 1.5 minutes or a high-efficiency particulate arresting filter was recommended [23]. Many ambulance infection control programs already suggested guidelines for an indepth program for sterilization, decontamination of material and equipment [23]. However, the actual adherence to these guidelines or the effect of these control programs remains unknown. In the setting of the present study, pre-hospital ambulances are operated by the fire department while inter-facility ambulances are operated by private companies or hospitals. According to the emergency medical service agency or ambulance authority, adherence to an infection control program could be variable. We do not know what kinds of screening and surveillance programs would be effective for ambulance infection control for each ambulance configuration.
This study had several limitations. The study was performed using a retrospective data review, which might result in the underestimation of the prevalence of TB, MRSA, and VRE. To determine the exact prevalence of these infections in the study hospital, we should test and culture the specimen for all patients of the study period. We know that the result cannot be generalized to all EDs because this study was from only a single tertiary teaching hospital ED. Future research should investigate the representative incidence and prevalence rate of across South Korea using data on the nationally notifiable communicable diseases that is collected by the Korea CDC. The tremendous efforts that have been made to improve surveillance of nosocomial infections like MRSA and VRE would be a good foundation for establishing preventive and public health policies. There were differences of severity such as admission and mortality rate, regardless of type of disease, between the pre-hospital ambulance group, inter-facility ambulance group, and non-ambulance group. The ORs of the ambulance-using groups might be overestimated if difference of disease severity between patients would be a potential confounder for positive carriage of TB, MRSA, and VRE. We could not conclude that the prevalence of these microorganism infections was associated with the direct probability of contamination to other patients using the ambulance; however, the data suggest that the high prevalence among patients who transported by ambulances may be a risk factor of ongoing community transmission because it can be a potential source of infection to the next patient who is transported by the ambulance. Future research should investigate the actual transmission rate by monitoring suspected cases that use ambulances and any rate of reduction that follows the initiation of an infection control program for ambulances.
In conclusion, ambulances can be a potential source of MRSA, VRE, and TB contamination. We found a much higher prevalence of those infections in the patient group transported from other hospitals, followed by the patient group transported by prehospital ambulances. Further study on the effectiveness of infection control programs should aim to identify the ways prehospital providers can reduce the risk of transmission of microorganisms among patients.
Notes
The authors have no conflicts of interest with the material presented in this paper.
This article is available at http://jpmph.org/.