Perceived Relevance of Educative Information on Public (Skin) Health: A Cross-sectional Questionnaire Survey
Article information
Abstract
Objectives
Unprotected leisure time exposure to ultraviolet radiation from the sun or artificial tanning beds is the most important environmental risk factor for melanoma, a malignant skin cancer with increasing incidences over the past decades. The aim of the present study was to assess the impact of skin health information provided by several sources and different publishing issues on knowledge, risk perception, and sun protective behavior of sunbathers.
Methods
A cross-sectional questionnaire survey was conducted among Austrian residents (n=563) spending leisure time outdoors in August 2010.
Results
Print media, television, and family were perceived as the most relevant sources of information on skin health, whereas the source physician was only ranked as fourth important source. Compared to other sources, information provided by doctors positively influenced participants' knowledge on skin risk and sun protective behavior resulting in higher scores in the knowledge test (p=0.009), higher risk perception (p<0.001), and more sun protection (p<0.001).
Regarding gender differences, internet was more often used by males as health information source, whereas females were more familiar with printed information material in general.
Conclusions
The results of this survey put emphasis on the demand for information provided by medical professionals in order to attain effective, long-lasting promotion of photoprotective habits.
INTRODUCTION
Ultraviolet (UV) radiation initiates damage of epidermal cells associated with skin tanning and is a causative factor for the development of the malignant skin cancer melanoma [1]. Since the early 1970s, an increase in incidence rates of melanoma has been observed worldwide, especially in fair-skinned populations and young females [2]. This alarming trend may root in personal habits regarding exposure to natural and artificial UV light, influenced by the common societal perception that a tanned skin is desirable and enhances attractiveness. Consequent lifelong sun protection and sunscreen use reduce the potential risk of cancer promotion and should be broadly addressed by health educative measures early in life [3].
Knowledge and beliefs of skin health promotion are influenced by various factors including health education campaigns and advertising as well as media and friends [4]. Thus, prevention of acute and chronic manifestations of UV light exposure could be increased with a limited amount of basic knowledge provided by counselling in general practice [5,6]. Therefore, information material designed to educate on Public (Skin) Health issues serve as important communication tools of decision-making in doctors-patients relationship and preventive medicine [7]. Preventive efforts reduce mid- and long-term costs for public medical care of all types of UV radiation-related skin diseases [8,9].
In Austria, a German-speaking country in central Europe, little is known on the public awareness and acceptance of country-wide available information material on tanning behavior and sun protection and their actual effect on knowledge and individual habits.
In the present cross sectional study, we explored the relevance of eight specific sources for information (print media, television, family, physician, internet, friends, radio, and school), and different providers of information material, i.e., indoor tanning parlours, health care providers, and sun screen producing companies, and their impact on knowledge, perceived risk estimation, and skin health behavior.
METHODS
Study Area and Study Population
The study was carried out at the Viennese banks of the River Danube in Austria. The recreation area was unrestricted with free public access. Data were collected at site in August 2010 with a total of 242 sun hours and daily air temperatures between 9.5℃ and 29.7℃ [10]. Study subjects were identified as appropriate population for evaluation of sun and skin health-associated issues for obviously spending leisure time outdoors in bright sunshine.
Male and female adults with adequate German language proficiency were eligible to participate in this questionnaire survey. Subjects encountered at the study area between noon and evening were addressed by professional interviewers at site. Verbal consent was obtained from participants and each interview took about 7 to 8 minutes to complete. Participation in the survey was voluntary, anonymous, and could be refused as well as discontinued at any time without giving reason.
The study was approved by the ethical committee of the Medical University Vienna, Austria (EK662/2010).
Questionnaire Design
Using a structured German-language questionnaire including in total 71 questions, we assessed sociodemographic characteristics, classification of skin type based on the Fitzpatrick phototyping scale as well as tanning and sun protective behavior [11]. Furthermore, the study assessed the influence of two variables comprising perceived relevance of information sources (print media, television, family, physician, internet, friends, radio, and school) and information publisher (indoor tanning parlours, health care providers, and sun screen producing companies), respectively, on sun protective behavior, sun risk estimation perception, and participants' knowledge on skin health.
Relevance of eight relevant information sources (print media, television, family, physician, internet, friends, radio, and school) was evaluated by the question "Which of the following sources of information about sun protection are relevant to you?", allowing multiple answers [12,13]. Ranking of these sources was performed by computing overall and gender-differentiated percentages of picked sources.
Further, publishing sources of educative materials were assessed using the multiple-answer-question "From where do you get your knowledge about sun protection?", offering the three choices information material provided by indoor tanning parlours, health care providers, and sun screen producing companies. Number of picked sources of information (n) was summed up and divided into two groups of either reporting few (0-3, n=350) or numerous (4-8, n=154) sources.
Sun Protective Behavior
Frequency of eight recommended sun protective behaviors including use of headgear, sun glasses, clothes, sun screen (at least SPF 15) avoiding sun between midday hours, staying in the shade, reapplying sun screen several times and after sweating or swimming was measured, using a five-point Likert scale ranging from "never" to "always" [14]. In order to calculate sum-scores on sun protective behavior, we generated a scale on sun protection comprising these eight items showing an acceptable internal consistency (Cronhbach's alpha: 0.73) [15]. For the covariate "sun protection", the mean of the sum score of this scale was computed.
Sun Risk Perception
We assessed participants' perceived or subjective perception of dangers of sun exposure regarding skin cancer, skin ageing, and overall risk of tanning, using a five-point Likert scale ranging from "no risk" to "very high risk." To calculate sum-scores on sun risk perception, we generated a scale on sun risk which consisted of three items, showing an internal consistency of Cronhbach's alpha: 0.64, which we assumed to be acceptable. For the covariate "risk perception," the mean of the sum score of these items was computed.
Knowledge on Skin Health
Participants' knowledge of important facts on sun exposure including indoor and outdoor UV-light exposure, skin cancer, sun screen, risks of sun tanning, was tested with a quiz comprising nine true-false questions, adapted from the literature [16-18]. To yield a knowledge score, we summed the number of correct responses to these nine items for generating the covariate "knowledge," resulting in a highest achievable score of nine correct answers.
Statistical Data Analysis
The collected data were statistically evaluated using Excel database (Microsoft, Seattle, WA, USA) and SPSS version 17.0 (SPSS Inc., Chicago, IL, USA). Single missing values with random distribution were tolerated without interpolation approaches to avoid loss of power. Univariate descriptive analysis was performed by chi-square test to evaluate associations in respect to gender differences regarding sources and publishing issues of information material. Concerning the knowledge score, comparisons of means were computed by independent samples t-test. For evaluating effects of information sources (independent variables; the source "physician" was compared to the other sources) and the summed amount of picked sources on the participants' individual behavior, multivariate analysis of variance was conducted with the dependant variables "knowledge," "risk perception," and "sun protection."
Spearman rank correlation (rs) was performed to measure the strength of the association between total amount of picked sources of information and publishing issues of information material. Level of significance was set at p=0.05.
RESULTS
A total of 680 people were conveniently approached. As 117 of those subjects refused to participate in the survey, the resulting response rate was 82.8%. Thus, final study subjects were 563. Basic data on the study population are summarized in Table 1. The average age of the participants (65.4% females), was 36.7 years, ranging from 18 to 83 years (males: mean, 35.6 years; SD, 13.9; females: mean, 37.28 years; SD, 15.6). Regarding education, about one third (32.5%) had at least a high school degree, and 35.8% had graduated from university.
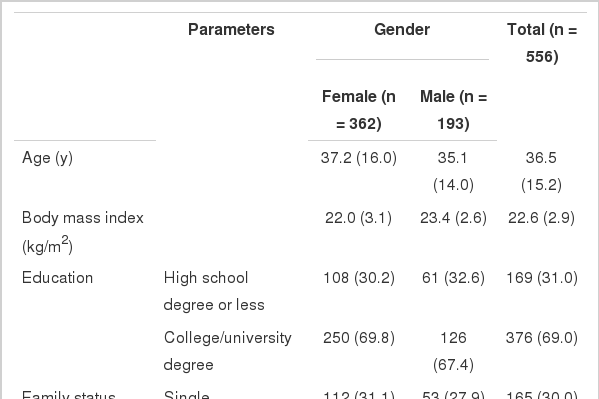
Basic characteristics of study population, stratified by gender
More than half of study participants (57.4%) classified their skin phototype as type III, whereas skin type I (1.8%), skin types II and IV (24.8% and 15.9%, respectively) were less frequently reported.
We assessed the relevance of information sources of educative material on skin health for female and male participants, respectively (Table 2). Significant gender differences were revealed regarding relevance of the information source "internet" (24.7% of the female participants versus 36.1% of the males, chi-square p-value=0.004) and according information material provided by sun screen producers (74.6% of the female participants versus 63.9% of the males, chi-square p-value=0.01).
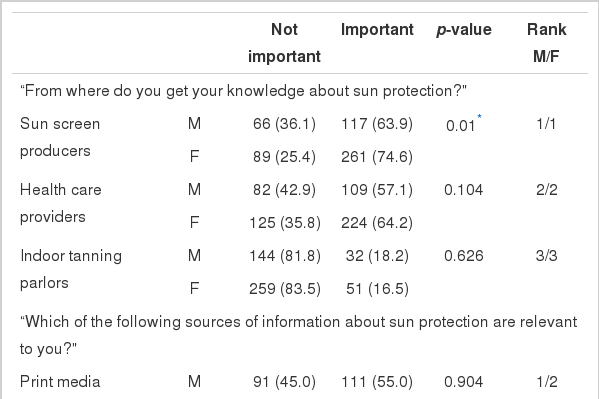
Ranking of relevance of information material on skin health by publisher and sources, stratified by gender, male (M) and female (F)
Ranking of sources of health information corresponding to their relevance revealed that the two most important sources of information on sunscreen issues were print media and television, holding each about one fifth of the total sample. Both male and female participants ranked "physician" as the fourth important source. Highlighting gender differences, male participants compared to females, were more likely to use the internet (rank 5, 10%) as a source of health information (p>0.01).
Mean knowledge score of issues relevant for skin health behavior was 7.80, SD 1.1. In congruence with the aforementioned results, participants who picked the physician as source of information, compared to participating people who did not, achieved higher point score in the knowledge test (mean, 7.97; SD, 0.9 compared to mean, 7.69; SD, 1.2; respectively), showed a higher risk perception (mean, 3.13; SD, 0.7 compared to mean, 2.87; SD, 0.7; respectively), and performed more sun protection (mean, 3.10; SD, 0.7 compared to mean, 2.90; SD, 0.7; respectively).
Participants' perceived relevance of "physician" in comparison with all the other sources (namely print media, television, family, internet, friends, radio, and school) was a significant contributor to knowledge on skin health (p=0.009), sun perception (p<0.001), and sun protection (p<0.001). In contrast, the summed amount of picked information sources did not significantly influence knowledge, sun risk perception, and sun protection (p>0.05) (Table 3).
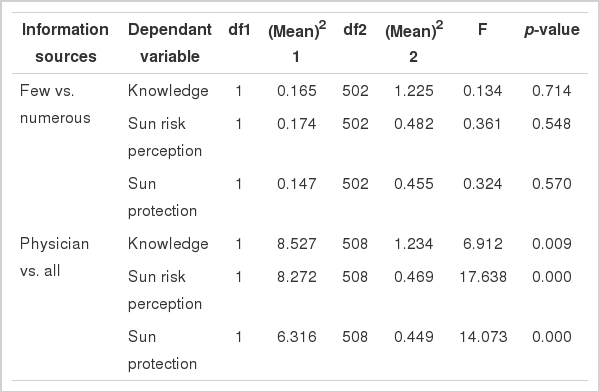
Results from multivariate analysis of variance for effects of information sources on study subjects’ knowledge, sun risk perception, and sun protection
The three defined types of materials were not fully correlated, but the information materials from sunscreen producers and indoor tanning companies were significantly associated (rs=0.161) (Table 4). Even though picking of the physician as a source of information was not correlated with other named sources, material from medical campaigns was associated with several sources of information-physician, family, friends (all p>0.01), and print media (p>0.05). Noteworthy, information material from sunscreen producers was neither related to the use of self-tanning lotions (rs=0.031) nor to medical information material (rs=-0.01), but showed a significant association with information provided by indoor tanning companies (rs=0.161).

Correlations between amount of picked sources of information and publisher of information material
DISCUSSION
The present study was conducted to assess the relevance of different sources as well as different media providing skin health information in Austria in order to identify new target-group specific information channels for target-group specific (e.g., gender) Public (Skin) Health promotion and skin cancer prevention. Additionally, we analyzed hypothesized associations between the perceived relevance of the source "physician" and skin health-related behaviour.
As a result, physicians were ranked only in fourth place as reliable source of information on sun and skin cancer issues. Print media, television, and family as information sources were ranked prior to physicians. This finding is consistent with results from Weinstein and co-workers, who reported a similar ranking for information sources: television, magazines, radio, dermatologists, and primary care physicians [19]. The comparison between relevance of the doctor as a source of information on skin health with other information sources analyzed how the specific source influenced skin health-related issues. Here, we report significantly better knowledge and thus, perception of skin risk factors as well as on sun protective behavior in the group of participants stating physicians as known, reliable source, indicating the profound and long-lasting effect of medical communication and counselling. These results on the favourable influence information provided by dermatologists and general practitioners were also found in a study performed by Suppa et al. [20].
In synopsis with previous publications stating gender differences in tanning behavior, our data suggested that the well-established differences in tanning habits of males and females may partly root in the type of information source males and females usually use [21,22]. The presented data provide evidence for significant gender differences of the perceived relevance regarding printed material from sunscreen producers (p=0.01) by females. Further, we reported a tendency that women were more likely to read printed information folders, whereas men were more likely to use the information source "internet" (p=0.004). Previous publications showed that information provided online was poor in quality and accuracy [23]. It may be considered as a disadvantage if patients retrieve health information online that could possibly hamper doctor-patient communication concerning professional education on tanning behavior.
However, people with more knowledge, higher risk perception, and better sun protective behavior could be more likely to know that a doctor is a trustworthy contact person with educative properties and professional knowledge on skin health issues [24]. In addition, presentation of educative content by using sun awareness posters was shown to achieve poor influence on patients' tanning behavior modifications compared to personal communication with medical professionals [25]. Remarkably, authors of a recent publication found poor sun risk knowledge and behavior of medical students in France, Europe, concluding that future medical professionals might not be the best channel for information on sun protection [26].
Motives of having or not having a tan are strongly influenced by the individual's concern of impaired attractiveness due to sun light rather than knowledge and perception of a possible skin cancer risk [27]. To achieve a modification of tanning habits towards sun protective behavior the perceived positive attitude of having a tanned skin has to be altered [12]. An emphasis on the advantages of reasonable sun exposure for the preservation of attractiveness and detailed description of drawbacks of unprotected UV-light exposure such as pigmentary abnormalities, skin dryness, and wrinkles could be more impressive than repeated alert of a future uncertain melanoma risk [28]. However, empathic communication may be the key to effective counselling on skin health promotion [29]. Education on skin health related issues could be easily integrated in doctor-patient communication, as the skin as a vital organ is obvious to the observer and not hidden like the viscera. Therefore, medical professions of all disciplines should be activated to assist dermatologists in the important subject of reducing UV light-associated skin diseases. The Public Health system could facilitate incorporating counselling on a more healthy lifestyle including tanning behavior into every day's medical practice by providing monetary resources and thus profiting from the long-term reduction of expenses [30].
Study limitations and strengths: Questionnaires were distributed during day time in summer. Therefore, people that principally avoided sun light or outdoor activity did scarcely participate in this study. Our data were self-reported introducing social desirability and non-response biases. As every person entering the outdoor study site was asked for participation, the study cohort was gender-imbalanced (65.4% females). However, the study area was highly frequented, with unrestricted year-round free public access. Therefore, participants reflected a current cross section of visitors at site.
As strength of the study, the present evaluation provided so far missing empiric material on the perceived significance of skin health information sources and material for the German-speaking country Austria. Questionnaires were deliberately provided only in German language, as we aimed to address the same target group as printed and online information material available and distributed in Austria.
The presented data suggest that physicians utilize their impact on skin health best possible in order to become the primary source for skin health promoting information. Moreover, medical professionals should be aware of the beneficial effect of skin health preventive attempts and serve as contact and reliable source of information on skin health issues.
Awareness of the challenges in patient empowerment should be raised in the public health care system in order to provide evidence-based online and printed information material. By providing adequate resources, educate medical students and doctors of various fields in positive health communication, the health care system could facilitate the process of implementing an effective and smooth flow of information in doctor-patient communication including target-group specific educative material.
ACKNOWLEDGEMENTS
We would like to give special thanks to Leo Pauzenberger and Alexander Hofmann for assistance in data collection on site. David Jungwirth, Gabriela Strasser, Ivana Dolezal, and Isabella Hämmerle were helpful in data processing.
Notes
The authors have no conflicts of interest with the material presented in this paper.