Articles
- Page Path
- HOME > J Prev Med Public Health > Volume 53(3); 2020 > Article
-
Special Section: COVID-19Original Article
Forecasting COVID-19 Transmission and Healthcare Capacity in Bali, Indonesia -
I Md Ady Wirawan1,2
 , Pande Putu Januraga1,3
, Pande Putu Januraga1,3 -
Journal of Preventive Medicine and Public Health 2020;53(3):158-163.
DOI: https://doi.org/10.3961/jpmph.20.152
Published online: April 29, 2020
1Department of Public Health and Preventive Medicine, Faculty of Medicine, Udayana University, Bali, Indonesia
2Travel Medicine Research Group, Health Research Centre, Institute for Research and Community Services, Udayana University, Bali, Indonesia
3Center for Public Health Innovation, Faculty of Medicine, Udayana University, Bali, Indonesia
- Corresponding author: Pande Putu Januraga, MD, DrPH Department of Public Health and Preventive Medicine, Faculty of Medicine, Udayana University, Jl. PB Sudirman, Bali 80361, Indonesia E-mail: januraga@unud.ac.id
Copyright © 2020 The Korean Society for Preventive Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Objectives
- In the current early phase of the coronavirus disease 2019 (COVID-19) outbreak, Bali needs to prepare to face the escalation of cases, with a particular focus on the readiness of healthcare services. We simulated the future trajectory of the epidemic under current conditions, projected the impact of policy interventions, and analyzed the implications for healthcare capacity.
-
Methods
- Our study was based on the first month of publicly accessible data on new confirmed daily cases. A susceptible, exposed, infected, recovered (SEIR) model for COVID-19 was employed to compare the current dynamics of the disease with those predicted under various scenarios.
-
Results
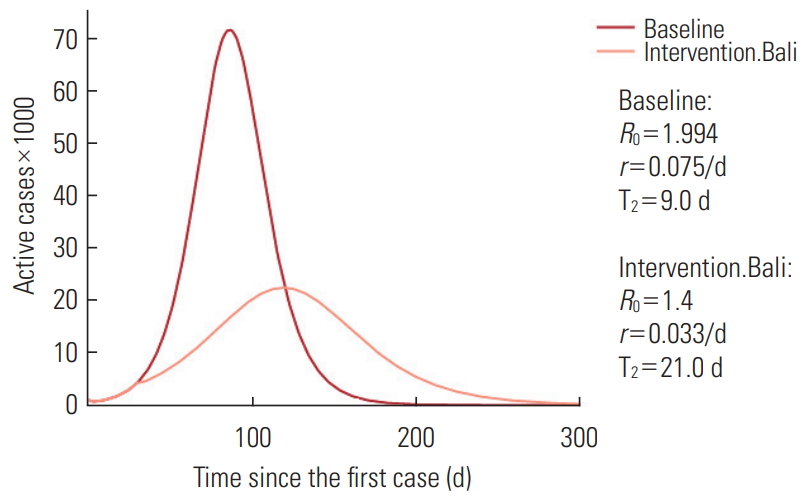
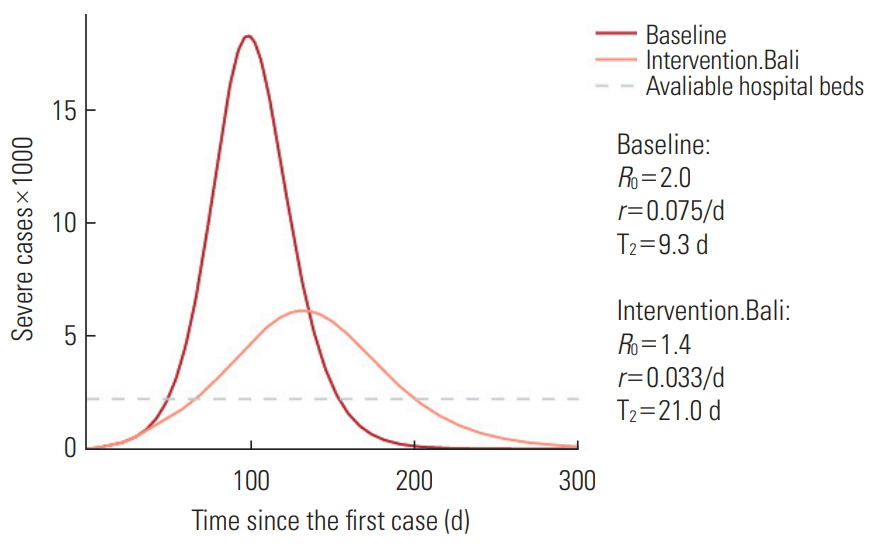
- The fitted model for the cumulative number of confirmed cases in Bali indicated an effective reproduction number of 1.4. Interventions have decreased the possible maximum number of cases from 71 125 on day 86 to 22 340 on day 119, and have prolonged the doubling time from about 9 days to 21 days. This corresponds to an approximately 30% reduction in transmissions from cases of mild infections. There will be 2780 available hospital beds, and at the peak (on day 132), the number of severe cases is estimated to be roughly 6105. Of these cases, 1831 will need intensive care unit (ICU) beds, whereas the number of currently available ICU beds is roughly 446.
-
Conclusions
- The healthcare system in Bali is in danger of collapse; thus, serious efforts are needed to improve COVID-19 interventions and to prepare the healthcare system in Bali to the greatest extent possible.
- Coronavirus disease 2019 (COVID-19) has become a pandemic and poses a major threat to public health in Indonesia. Bali is a province in Indonesia with a high risk of transmission due to international and domestic travel from areas affected by COVID-19. As of April 11, 2020, there were 75 cases of COVID-19 in Bali, predominantly among Indonesian migrant workers (mainly cruise ship workers) (60%), as well as locally imported cases from affected areas on other islands in Indonesia (20%) and cases in foreigners who traveled to Bali on vacation (10%) [1].
- Although only 10% of the current cases involved local transmission, the experiences of other settings demonstrate that Bali must prepare to face an escalation of cases, with a particular focus on the readiness of healthcare services, bearing in mind that 15-20% of cases will require hospital care and 5% of them will need intensive care, including ventilation [2]. Italy furnishes a vivid recent example of this issue, as a two-fold increase in cases within a short period of time resulted in insufficient space in the hospitals to accommodate the patients [3].
- Mathematical models of pandemic influenza have been used by policy-makers in many countries to inform estimates of disease severity and transmission characteristics, as well as to project the potential incidence trajectory of infected and fatal cases and the likely impact of control measures [4]. The same information is needed to determine the impact of non-medical interventions on the COVID-19 epidemic in Bali, and will facilitate better preparations and interventions.
- The aims of this study were to simulate the development of the COVID-19 epidemic in Bali with no interventions, to project the impact of the policy interventions that have been carried out so far on the trajectory of the COVID-19 epidemic in Bali based on the developments within 1 month since the first case was announced publicly, to describe the preparedness of health services in terms of the number of regular hospital beds and intensive care unit (ICU) beds available in Bali, and finally to make recommendations for policy-makers based on the results of this modeling.
INTRODUCTION
- Our study was based on the first month of publicly accessible data on new confirmed daily cases reported for the province of Bali from March 11, 2020 to April 10, 2020. An updated daily report can be seen at https://pendataan.baliprov.go.id. Based on the released data, we estimated the mean value of the effective reproduction number (Re) after the application of preventive measures in Bali. Furthermore, we compared the current dynamics of the disease with those expected in various scenarios, and assessed the effectiveness of the preventive measures in place. Lastly, we examined projections of hospital bed availability at the peak of the epidemic curve.
- We utilized a susceptible, exposed, infected, recovered (SEIR) model adapted to the complexity of COVID-19 spread using R version 3.6.3 (https://cran.r-project.org/src/base/R-3/). The SEIR COVID-19 scripts and code, which were originally developed by Hill and Phillips [5]. This code is an SEIR model for COVID-19 infection, including different clinical trajectories of infection, interventions to reduce transmission, and comparisons regarding healthcare capacity. The parameters used are presented in Table 1.
- Some important indicators analyzed in this study are explained as follows. The basic reproduction number (R0) is a mathematical term defined as the expected number of secondary infections arising from a single infectious individual in a susceptible population. In contrast, the effective Re is defined as the expected number of secondary infections arising from a single infectious individual in a susceptible population, after the introduction of preventive measures or interventions in a community [10].
- Ethics Statement
- The forecasting methods used freely available data from the public platform source with no primary data collection to human and animal subjects. Therefore, no institutional review board approval is needed.
METHODS
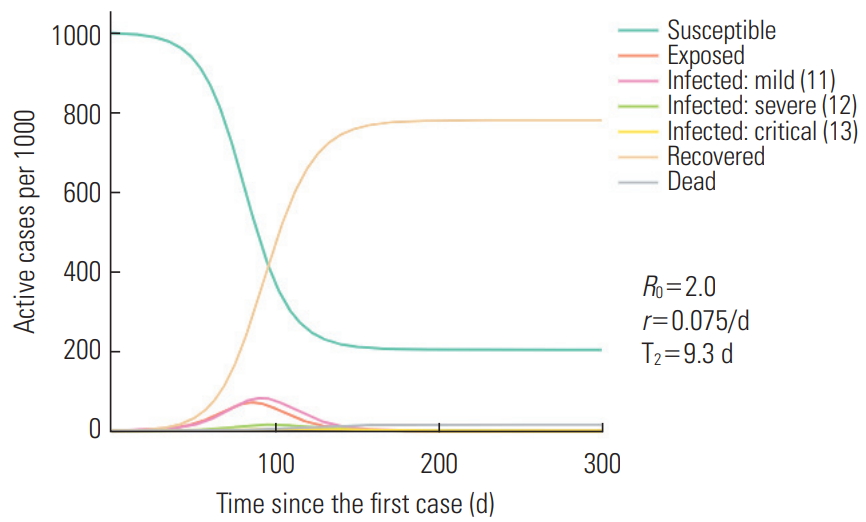
- The first simulation was conducted to assess the current situation with an R0 of 2.0, which is quite similar to the current figures in Indonesia, resulting in a doubling time of 9.3 days. Figure 1 indicates that, on the day when the simulation was performed (April 12, 2020), it was estimated that there were 3846 mild infections and that 4286 people were exposed without symptoms.
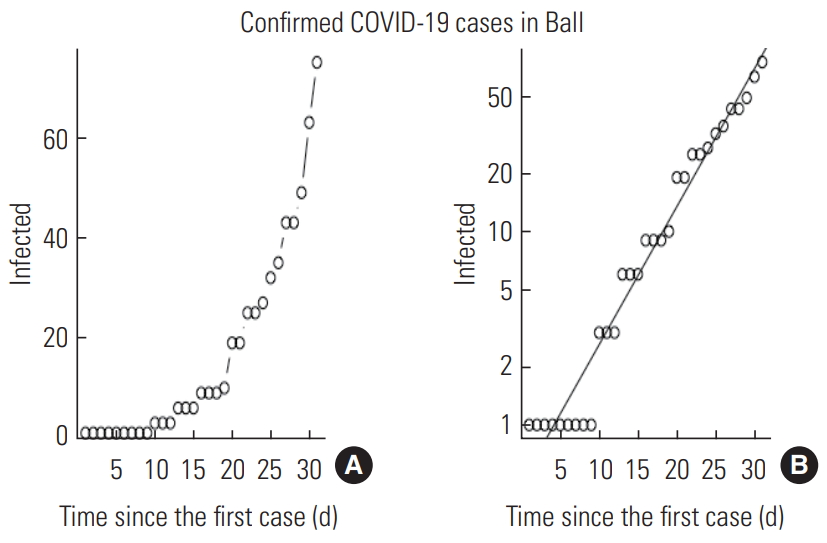
- The fitted model for the cumulative number of confirmed cases in Bali indicated an Re of 1.4 (Figure 2). This was used to estimate the effectiveness of the current preventive measures in Bali.
- We then simulated the spread of the disease using an R0 of 2.0 as the baseline and an Re of 1.4 for the situation in Bali after intervention.
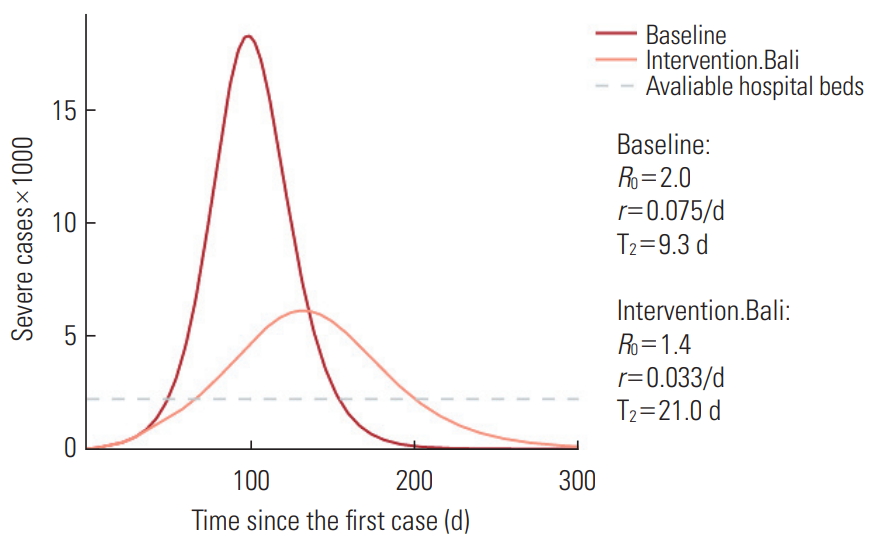
- Figure 3 indicates that the interventions implemented in Bali have decreased the possible maximum number of cases from 71 125 on day 86 to 22 340 cases on day 119, and prolonged the doubling time from about 9 days to 21 days. The model calculation resulted in an estimation that this situation approximately corresponds to a 30% reduction in transmission from cases of mild infections.
- Finally, we simulated the capacity of the healthcare system to care for patients with severe infections requiring hospitalization. As shown in Figure 4, there will be 2780 available hospital beds, and at the peak (on day 132), the number of severe cases is estimated to be roughly 6105. In addition, 1831 patients will need ICU beds, whereas the number of currenly available ICU beds in Bali is about 446 (assuming all ICU beds are emptied).
RESULTS
- Our model illustrates the impact of non-pharmaceutical interventions on the trajectory of the COVID-19 outbreak in Bali, Indonesia. Since the first case in Indonesia was announced in March 2, 2020, the provincial government of Bali has made an appeal to improve clean and healthy living behaviors by promoting social and physical distancing, implementing study and work from home policies, promoting masks for all, and implementing screening and quarantine policies, particularly for migrant workers returning to Bali. The details of preventive policies and measures that have been implemented in Bali are shown as below [1].
- • Formation of the COVID-19 Task Force before the first case was announced
- • Announcement of an emergency response and current implementation of an emergency alert
- • Starting on March 11, 2020, when case #25 in Indonesia was identified as a patient who was treated and died at Sanglah Hospital, the provincial government increased the intensity of the interventions
- • Augmentation of clean and healthy living behaviors and social distancing, which then became physical distancing
- • Disinfection of various public facilities (although this remains sporadic and unfocused)
- • Closure of elementary, middle, and high school as well as institutions of higher education since March 16, 2020
- • An appeal to work from home for offices and government agencies that was carried out more intensively at the end of March 2020
- • An appeal to delay or cancel domestic and international travel
- • Tightening of entrance of Bali since the end of March, including screening of Indonesian migrant workers with rapid antibody tests and quarantine
- • Prohibition of the Ogoh-ogoh festival (annual parade on the night before Balinese Nyepi, a day of silence in Bali where all people are obliged to stay home), and adding another day of prohibition of going out after Nyepi
- • A joint decision issued by the Indonesia Hinduism Society and Traditional Village Council on the implementation of Hindu ceremonies (Panca Yadnya) during the COVID-19 outbreak
- • Promotion of a face mask campaign for all people
- • Governor’s instructions for strengthening social restrictions and physical distancing
- • Designation of referral hospitals and a COVID-19 special hospital
- • Improvements in the screening and quarantine flow involving district/city governments
- • Formation of a Mutual Assistance Task Force at the village level
- The current policies and preventive measures implemented by the government of Bali and other related sectors have resulted in a 30% reduction in the risk of transmission from cases of mild infections. These interventions have had an impact on the decline of the Re of COVID-19 in Bali to 1.4, translating to a longer doubling time. However, assuming this outbreak is occurring via community spread [11], the modeling results imply that numerous COVID-19 cases will occur in Bali. Predictions of the outbreak trajectory and forecasting of demand for health facilities, particularly ICUs, have also been conducted in Italy, where they were proven to be correct in the following days [12]. Thus, without increasing the intensity of interventions at a larger scale, the capacity of health services will not be sufficient to handle the thousands of COVID-19 cases that will require treatment at hospitals and especially in ICUs. On the peak day, the number of severe cases is estimated to be approximately 6105, of which 1831 will need ICU beds. With the current bed and ICU availability, the healthcare system is in danger of collapse. Serious efforts are needed to improve COVID-19 preventive interventions and to prepare the healthcare system in Bali as much as possible.
- Based on the model we developed, our suggestions include any containment measures that could reduce susceptibility, exposure, or risk of infection and any measures to prepare healthcare facilities. First, to reduce the proportion of the susceptible population, we suggest that the government of Bali should tighten the implementation of social restrictions and examine the possibility of implementing large-scale social restrictions, known as PSBB in Indonesia. PSBB could be implemented at the district and provincial levels with approval from Ministry of Health of Indonesia. The key components of PSBB are the closure of schools and working facilities (including factories), restriction of public activities (including religious ceremonies), restriction of public transportation, and other restrictions (including defense and security activities). An additional component of PSBB is the ability of local government to deploy law enforcement [13].
- Second, to reduce exposure, preventive measures for reducing contact duration with asymptomatic but exposed individuals are needed [14]. This includes increasing the capacity of reverse-transcription polymerase chain reaction tests, at least for screening exposed populations [15], such as those categorized as people under monitoring (known as ODP in Indonesia) and asymptomatic close contacts, as well as travelers and Indonesian migrant workers. The government of Bali is currently screening migrant workers using a rapid antibody test, and additional consideration should be given to false negatives, the exact timing of testing, and improving quarantine procedures involving district governments in Bali. It is also paramount to tighten air and sea entrances, because there is a high risk of imported transmission from other red zone areas on other Indonesian islands, where screening and quarantine procedures also need to be applied.
- The risk of infection can also be reduced by intensifying health promotion measures even at the village-level, promoting the importance of washing hands, wearing masks, and maintaining physical distance. Furthermore, transmission in healthcare facilities can be reduced by providing adequate personal protective equipment for health workers from primary care to secondary and tertiary referral hospitals. A report from Italy revealed that 8.4% of hospitalized COVID-19 patients were healthcare workers at hospitals [3]. As the epidemic is growing, more patients will require hospitalization, meaning that an inability to increase the capacity of healthcare facilities could lead to the possibility of hospitals becoming the epicenter of COVID-19 transmission.
- However, the collapse of the healthcare system can be anticipated by improving healthcare system capacity and financing to be more flexible, with appropriate consideration of exceptional emergencies such as the preparation of more hospital beds, even in field or temporary hospitals. Furthermore, solid partnerships between the private and public sector should be formalized, as only 2 private hospitals in Bali are currently prepared to provide care for COVID-19 patients. The provincial government should categorize current COVID-19 referral hospitals according to the level of supporting technology and health personnel capacity, and should play a role in designing referral flow and procedures. In addition, mapping the availability of health workers with special qualifications needed for COVID-19 services and mobilizing them effectively for COVID-19 case management in Bali are paramount in preparing the healthcare system for the increase in severe and critical cases. These improvements in hospitals’ capacity will require planning and financing for the recruitment of qualified human resources [16,17].
- Lastly, within the current testing capacity in Bali, Indonesia, we acknowledge that there may be a delay before symptom appearance due to the incubation period, thereby resulting in a delayed confirmation of cases. Incorporating delays stemming from the natural history of the infection and reporting processes in the model might provide different figures, with different consequences in terms of preparing the health system and strategies to improve public health measures to contain the epidemic [18]. As more data become available for Bali, it will be possible to refine these estimates; however, for now, these modeling results have helped us to understand the effectiveness of current interventions and the likely trajectory of the epidemic in response to interventions during the upcoming months, thereby enabling better containment strategies.
DISCUSSION
-
CONFLICT OF INTEREST
The authors have no conflicts of interest associated with the material presented in this paper.
-
FUNDING
None.
Notes
ACKNOWLEDGEMENTS
-
AUTHOR CONTRIBUTIONS
Conceptualization: IMAW, PPJ. Data curation: IMAW, PPJ. Formal analysis: IMAW. Funding acquisition: None. Methodology: IMAW. Writing - original draft: IMAW. Writing - review & editing: IMAW, PPJ.
Notes

| Parameter | Frequency | Source |
|---|---|---|
| Population of Bali (n) | 4 300 000 | BPS projection in 2019 [6] |
| Incubation period (d) | 5 | Linton et al. 2020 [7] |
| Duration of mild infections (d) | 6 | Woelfel et al. 2020 [8] |
| % of symptomatic infections that are severe | 15.0 | Wu et al. 2020 [2] |
| % of symptomatic infections that are critical | 5.0 | Wu et al. 2020 [2] |
| Initial infection | 1 | Bali Province COVID-19 [1] |
| Total hospital beds per 1000 people | 1.62 | The number of hospital beds in Bali is 6948: hospital database system [9] |
| Average % occupancy of hospital beds | 60.0 | Hospital database system [9] |
| Total ICU beds per 1000 people | 0.1 | The number of ICU beds in Bali is 446 [9] |
- 1. Provincial Government of Bali. Bali province response COVID-19 [cited 2020 May 20]. Available from: https://infocorona.baliprov.go.id/
- 2. Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA 2020;323(13):1239-1242ArticlePubMedPDF
- 3. Lazzerini M, Putoto G. COVID-19 in Italy: momentous decisions and many uncertainties. Lancet Glob Health 2020;8(5):e641-e642ArticlePubMedPMC
- 4. Van Kerkhove MD, Ferguson NM. Epidemic and intervention modelling—a scientific rationale for policy decisions? Lessons from the 2009 influenza pandemic. Bull World Health Organ 2012;90(4):306-310ArticlePubMedPMC
- 5. Hill A, Phillips B. SEIR_COVID19 [cited 2020 Apr 20]. Available from: https://github.com/alsnhll/SEIR_COVID19
- 6. Statistics of Bali Province. Population projection of Bali province by regency/municipality and gender, 2011-2020. [cited 2020 May 20]. Available from: https://bali.bps.go.id/dynamictable/2016/05/13/19/proyeksi-penduduk-provinsi-balimenurut-kabupaten-kota-dan-jenis-kelamin-2011-2020.html
- 7. Linton NM, Kobayashi T, Yang Y, Hayashi K, Akhmetzhanov AR, Jung SM, et al. Incubation period and other epidemiological characteristics of 2019 novel coronavirus infections with right truncation: a statistical analysis of publicly available case data. J Clin Med 2020;9(2):538ArticlePubMedPMC
- 8. Woelfel R, Corman VM, Guggemos W, Seilmaier M, Zange S, Mueller MA, et al. Clinical presentation and virological assessment of hospitalized cases of coronavirus disease 2019 in a travel-associated transmission cluster. medRxiv 2020. doi: https://doi.org/10.1101/2020.03.05.20030502Article
- 9. Ministry of Health of Indonesia. Indonesian hospital database system. 2019 [cited 2020 May 20]. Available from: http://sirs.yankes.kemkes.go.id/sirs/login.php (Indonesian)
- 10. Heffernan JM, Smith RJ, Wahl LM. Perspectives on the basic reproductive ratio. J R Soc Interface 2005;2(4):281-293ArticlePubMedPMC
- 11. Wilder-Smith A, Chiew CJ, Lee VJ. Can we contain the COVID-19 outbreak with the same measures as for SARS? Lancet Infect Dis 2020;20(5):e102-e107ArticlePubMedPMC
- 12. Grasselli G, Pesenti A, Cecconi M. Critical care utilization for the COVID-19 outbreak in Lombardy, Italy: early experience and forecast during an emergency response. JAMA 2020;323(16):1545-1546ArticlePubMedPDF
- 13. Government of Indonesia. Government Regulation No. 21, year 2020 on large scale social restriction. [cited 2020 Apr 20]. Available from: https://jdih.setkab.go.id/PUUdoc/176085/PP_Nomor_21_Tahun_2020.pdf (Indonesian)
- 14. Bai Y, Yao L, Wei T, Tian F, Jin DY, Chen L, et al. Presumed asymptomatic carrier transmission of COVID-19. JAMA 2020;323(14):1406-1407ArticlePubMedPMCPDF
- 15. Berger ZD, Evans NG, Phelan AL, Silverman RD. COVID-19: control measures must be equitable and inclusive. BMJ 2020;368: m1141ArticlePubMed
- 16. Legido-Quigley H, Asgari N, Teo YY, Leung GM, Oshitani H, Fukuda K, et al. Are high-performing health systems resilient against the COVID-19 epidemic? Lancet 2020;395(10227):848-850ArticlePubMedPMC
- 17. Armocida B, Formenti B, Ussai S, Palestra F, Missoni E. The Italian health system and the COVID-19 challenge. Lancet Public Health 2020;5(5):e253ArticlePubMedPMC
- 18. Kucharski AJ, Russell TW, Diamond C, Liu Y, Edmunds J, Funk S, et al. Early dynamics of transmission and control of COVID-19: a mathematical modelling study. Lancet Infect Dis 2020;20(5):553-558ArticlePubMedPMC
REFERENCES
Figure & Data
References
Citations
- The Impacts of Medical Resources on Emerging Self-Limiting Infectious Diseases
Dayong Zhou, Liyan Gao, Qiuhui Pan, Mingfeng He
Applied Sciences.2022; 12(9): 4255. CrossRef - Transmission dynamics model and the coronavirus disease 2019 epidemic: applications and challenges
Jinxing Guan, Yang Zhao, Yongyue Wei, Sipeng Shen, Dongfang You, Ruyang Zhang, Theis Lange, Feng Chen
Medical Review.2022; 2(1): 89. CrossRef - Comprehensive Travel Health Education for Tour Guides: Protocol for an Exploratory Sequential Mixed Methods Research
Ni Made Sri Nopiyani, Pande Putu Januraga, I Md Ady Wirawan, I Made Bakta
JMIR Research Protocols.2022; 11(5): e33840. CrossRef - Seroprevalence of SARS-CoV-2 antibodies in Bali Province: Indonesia shows underdetection of COVID-19 cases by routine surveillance
Anak A. S. Sawitri, Putu C. D. Yuliyatni, Putu A. S. Astuti, Emita Ajis, Endang B. Prasetyowati, Husni, Juliette Morgan, Jennifer Mika, Catharina Y. Praptiningsih, Amalya Mangiri, Ester Mulyadi, Rintis Noviyanti, Leily Trianty, William A. Hawley, Gathsau
PLOS Global Public Health.2022; 2(8): e0000727. CrossRef - Correlation of Demographics, Healthcare Availability, and COVID-19 Outcome: Indonesian Ecological Study
Gede Benny Setia Wirawan, Pande Putu Januraga
Frontiers in Public Health.2021;[Epub] CrossRef - Perceived Social Norms as Determinants of Adherence to Public Health Measures Related to COVID-19 in Bali, Indonesia
Putu Ayu Indrayathi, Pande Putu Januraga, Putu Erma Pradnyani, Hailay Abrha Gesesew, Paul Russel Ward
Frontiers in Public Health.2021;[Epub] CrossRef - Prevalence of Depression, Anxiety, and Stress Among Repatriated Indonesian Migrant Workers During the COVID-19 Pandemic
Ngakan Putu Anom Harjana, Pande Putu Januraga, Putu Ayu Indrayathi, Hailay Abrha Gesesew, Paul Russell Ward
Frontiers in Public Health.2021;[Epub] CrossRef - Determinants of Mental Health and Practice Behaviors of General Practitioners During COVID-19 Pandemic in Bali, Indonesia: A Cross-sectional Study
Firman Parulian Sitanggang, Gede Benny Setia Wirawan, I Md Ady Wirawan, Cokorda Bagus Jaya Lesmana, Pande Putu Januraga
Risk Management and Healthcare Policy.2021; Volume 14: 2055. CrossRef - Improving Public Access to COVID-19 Pandemic Data in Indonesia for Better Public Health Response
Pande Putu Januraga, Ngakan Putu Anom Harjana
Frontiers in Public Health.2020;[Epub] CrossRef - Modeling the transmission dynamics of COVID-19 epidemic: a systematic review
Jinxing Guan, Yongyue Wei, Yang Zhao, Feng Chen
The Journal of Biomedical Research.2020; 34(6): 422. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite